Aripiprazole lauroxil
Aripiprazole lauroxil (brand name Aristada) is a long-acting injectable atypical antipsychotic that was developed by Alkermes.[1][2][3] It is an N-acyloxymethyl prodrug of aripiprazole that is administered via intramuscular injection once every four to eight weeks for the treatment of schizophrenia.[1][2][3] Aripiprazole lauroxil was approved by the U.S. FDA on 5 October 2015.[4][5]
 | |
| Clinical data | |
|---|---|
| Trade names | Aristada |
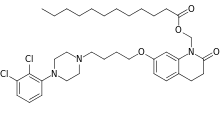
| Other names | ALKS-9070; ALKS-9072; RDC-3317; Dodecanoic acid-[7-[4-[4-(2,3-dichlorophenyl)-1-piperazinyl]butoxy]-3,4-dihydro-2-oxo-1(2H)-quinolinyl]methyl ester |
| Routes of administration | Intramuscular |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| ChemSpider | |
| UNII | |
| KEGG | |
| CompTox Dashboard (EPA) | |
| ECHA InfoCard | 100.261.570 |
| Chemical and physical data | |
| Formula | C36H51Cl2N3O4 |
| Molar mass | 660.72 g·mol−1 |
| 3D model (JSmol) | |
| |
| |
Medical uses
Aripiprazole lauroxil extended release injection gained FDA approval in 2015 as a treatment for adults suffering from schizophrenia. Like any long-term acting injectable, aripiprazole lauroxil provides assurance to families and health care professionals that patients receive therapeutic medication throughout the day.[6]
Aripiprazole lauroxil is injected into the arm or buttocks of a patient by a health care professional once every four to six weeks. Aripiprazole lauroxil is a longer-lasting and injectable version of the schizophrenia pill aripiprazole, which means that the treatment is available in two doses. Aripiprazole lauroxil, along with other drugs in its family, are not approved for treatment of elderly patients with dementia-related psychosis.[6][7]
Schizophrenia
The approval of aripiprazole lauroxil from the Food and Drug Administration in 2015 was solely for the treatment of schizophrenia in adults. The ability to supplement aripiprazole lauroxil with oral supplements of aripiprazole allows for dosing flexibility, which is important for the treatment of schizophrenia, as symptoms and intensity of the disease vary greatly from patient to patient. Additionally, as in concurrence with its sister drug aripiprazole, aripiprazole lauroxil is similar in effect of typical antipsychotic drugs.[8] In the sister drug aripiprazole, side effects for patients were less frequently extrapyramidal than most antipsychotic drugs.
Side effects
The most common side effects are akathisia. According to the drug’s warning label and safety information, the side effects are large in variety.[9]
The complete list of side effects include: akathisia, Contraindication Cerebrovascular Adverse Reactions (Including Stroke), Neuroleptic Malignant Syndrome, Tardive Dyskinesia, metabolic changes, Hyperglycemia/Diabetes Mellitus, Dyslipidemia, weight gain, Orthostatic Hypotension, Leukopenia, Neutropenia, Agranulocytosis, seizures, potential for Cognitive and Motor Impairment, difficulties with body temperature regulation, Dysphagia, Injection-Site Reactions (rash, swelling, redness, irritation at the point of injection), Dystonia and pregnancy and nursing complications.[10]
Discontinuation
The British National Formulary recommends a gradual withdrawal when discontinuing antipsychotics to avoid acute withdrawal syndrome or rapid relapse.[11] Symptoms of withdrawal commonly include nausea, vomiting, and loss of appetite.[12] Other symptoms may include restlessness, increased sweating, and trouble sleeping.[12] Less commonly there may be a felling of the world spinning, numbness, or muscle pains.[12] Symptoms generally resolve after a short period of time.[12]
There is tentative evidence that discontinuation of antipsychotics can result in psychosis.[13] It may also result in reoccurrence of the condition that is being treated.[14] Rarely tardive dyskinesia can occur when the medication is stopped.[12]
Overdosing
The largest known case of ingestion with a known outcome involved a 1260 mg of oral aripiprazole, 42 times the recommended dose. The patient survived and fully recovered.
Common adverse reactions, reported in at least 5% of overdose cases, included vomiting, somnolence, and tremor. Other clinically important signs and symptoms of overdoses include acidosis, aggression, atrial fibrillation, bradycardia, coma, confusion, convulsion, depressed level of consciousness, hypertension, hypokalemia, hypotension, lethargy, loss of consciousness, pneumonia aspiration, respiratory arrest, status epilepticus, and tachycardia.[6]
Pharmacology
Mechanism of action
Arristada is injected into the intramuscles as an atypical antipsychotic. In one 12-week clinical trial involving 622 participants, the efficacy of extended aripiprazole was demonstrated.[7][10] Its mechanism of action is not completely known, but is thought to be converted by enzyme-mediated hydrolysis to N-hydroxymethyl aripirazole. The hydroxymethyl aripirazole is then hydrolysed to aripiprazole. Efficacy could be mediated through a combination of partial agonist activity D2 and 5-HT1A receptors and antagonist activity at 5-HT2A receptors. Since it is a newly approved drug by the FDA, many validation of mechanisms of action are still being studied.[10]
Pharmacodynamics
Aripiprazole exhibits high affinity for serotonin 5-HT1A, 5-HT2A receptors, dopamine D2, and dopamine D3. Moderate affinity is exhibited for serotonin 5-HT7, alpha1-adrenergic, dopamine D4, histamine H1, and serotonin re-uptake site. No affinity for cholinergic muscarinic receptors have been found.[10]
Pharmacokinetics
Aristada’s activity in the body is due to aripiprazole and also dehydro-aripiprazole. Dehydro-aripirazole has been shown to have affinities for D2 receptors. These D2 receptors have similarities to aripiprazole whereas they represent 30-40% of exposure of aripiprazole in plasma.
After 5 to 6 days of the single intramuscular injection appearance of aripiprazole in circulation, it additionally will be released for 36 days. In the fourth monthly injection, consecutive doses of Aristada will reach steady-state. With additional supplements of the oral aripiprazole at a dosage of 21 days during the first dose of Aristada, aripiprazole concentrations within 4 days can reach therapeutic levels.[10]
| Medication | Brand name | Class | Vehicle | Dosage | Tmax | t1/2 single | t1/2 multiple | logPc | Ref |
|---|---|---|---|---|---|---|---|---|---|
| Aripiprazole lauroxil | Aristada | Atypical | Watera | 441–1064 mg/4–8 weeks | 24–35 days | ? | 54–57 days | 7.9–10.0 | |
| Aripiprazole monohydrate | Abilify Maintena | Atypical | Watera | 300–400 mg/4 weeks | 7 days | ? | 30–47 days | 4.9–5.2 | |
| Bromperidol decanoate | Impromen Decanoas | Typical | Sesame oil | 40–300 mg/4 weeks | 3–9 days | ? | 21–25 days | 7.9 | [15] |
| Clopentixol decanoate | Sordinol Depot | Typical | Viscoleob | 50–600 mg/1–4 weeks | 4–7 days | ? | 19 days | 9.0 | [16] |
| Flupentixol decanoate | Depixol | Typical | Viscoleob | 10–200 mg/2–4 weeks | 4–10 days | 8 days | 17 days | 7.2–9.2 | [16][17] |
| Fluphenazine decanoate | Prolixin Decanoate | Typical | Sesame oil | 12.5–100 mg/2–5 weeks | 1–2 days | 1–10 days | 14–100 days | 7.2–9.0 | [18][19][20] |
| Fluphenazine enanthate | Prolixin Enanthate | Typical | Sesame oil | 12.5–100 mg/1–4 weeks | 2–3 days | 4 days | ? | 6.4–7.4 | [19] |
| Fluspirilene | Imap, Redeptin | Typical | Watera | 2–12 mg/1 week | 1–8 days | 7 days | ? | 5.2–5.8 | [21] |
| Haloperidol decanoate | Haldol Decanoate | Typical | Sesame oil | 20–400 mg/2–4 weeks | 3–9 days | 18–21 days | 7.2–7.9 | [22][23] | |
| Olanzapine pamoate | Zyprexa Relprevv | Atypical | Watera | 150–405 mg/2–4 weeks | 7 days | ? | 30 days | – | |
| Oxyprothepin decanoate | Meclopin | Typical | ? | ? | ? | ? | ? | 8.5–8.7 | |
| Paliperidone palmitate | Invega Sustenna | Atypical | Watera | 39–819 mg/4–12 weeks | 13–33 days | 25–139 days | ? | 8.1–10.1 | |
| Perphenazine decanoate | Trilafon Dekanoat | Typical | Sesame oil | 50–200 mg/2–4 weeks | ? | ? | 27 days | 8.9 | |
| Perphenazine enanthate | Trilafon Enanthate | Typical | Sesame oil | 25–200 mg/2 weeks | 2–3 days | ? | 4–7 days | 6.4–7.2 | [24] |
| Pipotiazine palmitate | Piportil Longum | Typical | Viscoleob | 25–400 mg/4 weeks | 9–10 days | ? | 14–21 days | 8.5–11.6 | [17] |
| Pipotiazine undecylenate | Piportil Medium | Typical | Sesame oil | 100–200 mg/2 weeks | ? | ? | ? | 8.4 | |
| Risperidone | Risperdal Consta | Atypical | Microspheres | 12.5–75 mg/2 weeks | 21 days | ? | 3–6 days | – | |
| Zuclopentixol acetate | Clopixol Acuphase | Typical | Viscoleob | 50–200 mg/1–3 days | 1–2 days | 1–2 days | 4.7–4.9 | ||
| Zuclopentixol decanoate | Clopixol Depot | Typical | Viscoleob | 50–800 mg/2–4 weeks | 4–9 days | ? | 11–21 days | 7.5–9.0 | |
| Note: All by intramuscular injection. Footnotes: a = Microcrystalline or nanocrystalline aqueous suspension. b = Low-viscosity vegetable oil (specifically fractionated coconut oil with medium-chain triglycerides). c = Predicted, from PubChem and DrugBank. Sources: Main: See template. | |||||||||
Dosing
Aristada can be administered in three dosages of 441 mg, 662 mg and 882 mg. The smallest dosage can be injected in the Deltoid or Gluteus of the patient, while the higher doses must be injected into the Gluteus. Dosages of 441 mg or 662 mg must be repeated once every four weeks, while the dosage of 882 mg must be repeated once every six weeks.[9]
The dosages are determined based on the daily needs of the specific patient, but the timing and injection sites are not based on the needs of the patient and correspond to the amount in each dose.[7]
Early dosing
Aristada dosing is recommended to occur once every four weeks for doses of 441 mg or 662 mg. The recommended dosing for 882 mg is once every six weeks. These durations between doses should be maintained as much as possible. An Aristada injection should not be given any earlier than at least 14 days after the most recent injection.[8]
| Dose | Dosing Frequency | Site of Injection |
|---|---|---|
| 441 mg | Monthly | Deltoid or Gluteal |
| 662 mg | Monthly | Gluteal |
| 882 mg | Every Six Weeks | Gluteal |
| 1064 mg | Every Eight Weeks | Gluteal |
Missed doses
When a dose is missed, administer the next injection of aripiprazole lauroxil as soon as possible. It is important to keep the timing of the administration of the drug somewhat regular, as irregular dosing can produce sometimes unpredictable effects on the patient. If the length of time since an injection exceeds the length of time as listed in the following table, use oral Aripiprazole supplementation with the next aripiprazole lauroxil injection as listed:[8]
| Dose of Patient's Last aripiprazole lauroxil Injection | No Oral Supplementation Required | Supplement for 7 Days | Supplement for 21 Days |
|---|---|---|---|
| Monthly 441 mg | 6 weeks or less | 6–7 weeks | 7 weeks or more |
| Monthly 662 mg | 8 weeks or less | 8–12 weeks | 12 weeks or more |
| Monthly 882 mg | 8 weeks or less | 8–12 weeks | 12 weeks or more |
| 882 mg every six weeks | 8 weeks or less | 8–12 weeks | 12 weeks or more |
Dose adjustments
Once stabilized on aripiprazole, people taking CYP2D6 or CYP3A4 inhibitors or CYP3A4 inducers should refer to the dosing recommendations below, there are no dosage changes recommended for aripiprazole lauroxil if CYP450 modulators are added for less than two weeks.[8]
| Concomitant Medicine | Dose Changes for aripiprazole lauroxil |
|---|---|
| Strong CYP3A4 Inhibitor | Reduce the dosage of aripiprazole lauroxil to the next lowest dose, do not lower dose if the patient is already taking the lowest dosage of 441 mg, if tolerated. |
| Strong CYP2D6 Inhibitor | Reduce the dosage of aripiprazole lauroxil to the next lowest dose, do not change for those taking 441 mg dose, if tolerated. |
| Both Strong CYP3A4 Inhibitor
and Strong CYP2D6 Inhibitor |
No dosage adjustment necessary for patients taking 441 mg, if tolerated. Avoid use for patients taking the 662 mg or 882 mg dose. |
| CYP3A4 Inducers | No dose adjustment is necessary for patients taking the 662 mg or 882 mg dose. Increase the dosage for patients taking 441 mg to 662 mg. |
References
- Rohde M, M Rk N, Håkansson AE, Jensen KG, Pedersen H, Dige T, J Rgensen EB, Holm R (2014). "Biological conversion of aripiprazole lauroxil - An N-acyloxymethyl aripiprazole prodrug". Results Pharma Sci. 4: 19–25. doi:10.1016/j.rinphs.2014.04.002. PMC 4050360. PMID 25756003.
- Turncliff R, Hard M, Du Y, Risinger R, Ehrich EW (2014). "Relative bioavailability and safety of aripiprazole lauroxil, a novel once-monthly, long-acting injectable atypical antipsychotic, following deltoid and gluteal administration in adult subjects with schizophrenia". Schizophr. Res. 159 (2–3): 404–10. doi:10.1016/j.schres.2014.09.021. PMID 25266547.
- Meltzer HY, Risinger R, Nasrallah HA, Du Y, Zummo J, Corey L, Bose A, Stankovic S, Silverman BL, Ehrich EW (2015). "A randomized, double-blind, placebo-controlled trial of aripiprazole lauroxil in acute exacerbation of schizophrenia". J Clin Psychiatry. 76 (8): 1085–90. doi:10.4088/JCP.14m09741. PMID 26114240.
- Citrome L (2015). "Aripiprazole Long-Acting Injectable Formulations for Schizophrenia: Aripiprazole Monohydrate and Aripiprazole Lauroxil". Expert Rev Clin Pharmacol. 9 (2): 169–86. doi:10.1586/17512433.2016.1121809. PMID 26573020.
- "Aristada intramuscular : Uses, Side Effects, Interactions, Pictures, Warnings & Dosing - WebMD". WebMD. Retrieved 2016-04-18.
- "New Medical Devices". Pharmacy and Therapeutics. 40 (11): 716–774. 2015-11-01. ISSN 1052-1372. PMC 4634342. PMID 26609204.
- "Aristada". Drugs.com.
- "ARISTADA (aripiprazole lauroxil) | Treatment Prescribing Information". aristada.com. Archived from the original on 2016-04-03. Retrieved 2016-04-18.
- "DailyMed - ARISTADA- aripiprazole lauroxil injection, suspension, extended release". dailymed.nlm.nih.gov. Retrieved 2016-04-18.
- Joint Formulary Committee, BMJ, ed. (March 2009). "4.2.1". British National Formulary (57 ed.). United Kingdom: Royal Pharmaceutical Society of Great Britain. p. 192. ISBN 978-0-85369-845-6.
Withdrawal of antipsychotic drugs after long-term therapy should always be gradual and closely monitored to avoid the risk of acute withdrawal syndromes or rapid relapse.
- Haddad, Peter; Haddad, Peter M.; Dursun, Serdar; Deakin, Bill (2004). Adverse Syndromes and Psychiatric Drugs: A Clinical Guide. OUP Oxford. p. 207–216. ISBN 9780198527480.
- Moncrieff J (July 2006). "Does antipsychotic withdrawal provoke psychosis? Review of the literature on rapid onset psychosis (supersensitivity psychosis) and withdrawal-related relapse". Acta Psychiatrica Scandinavica. 114 (1): 3–13. doi:10.1111/j.1600-0447.2006.00787.x. PMID 16774655.
- Sacchetti, Emilio; Vita, Antonio; Siracusano, Alberto; Fleischhacker, Wolfgang (2013). Adherence to Antipsychotics in Schizophrenia. Springer Science & Business Media. p. 85. ISBN 9788847026797.
- Parent, M., Toussaint, C., & Gilson, H. (1983). Long-term treatment of chronic psychotics with bromperidol decanoate: clinical and pharmacokinetic evaluation. Current Therapeutic Research, 34(1), 1–6. https://scholar.google.com/scholar?cites=10379409109713994773
- Jørgensen A, Overø KF (1980). "Clopenthixol and flupenthixol depot preparations in outpatient schizophrenics. III. Serum levels". Acta Psychiatr Scand Suppl. 279: 41–54. doi:10.1111/j.1600-0447.1980.tb07082.x. PMID 6931472.
- Reynolds, J. E. F. (1993). Anxiolytic sedatives, hypnotics and neuroleptics. Martindale: The Extra Pharmacopoeia, 30th Edition (pp. 364–623). Pharmaceutical Press, London. https://scholar.google.com/scholar?cluster=8335042449033257176
- Ereshefsky L, Saklad SR, Jann MW, Davis CM, Richards A, Seidel DR (May 1984). "Future of depot neuroleptic therapy: pharmacokinetic and pharmacodynamic approaches". J Clin Psychiatry. 45 (5 Pt 2): 50–9. PMID 6143748.
- Curry SH, Whelpton R, de Schepper PJ, Vranckx S, Schiff AA (April 1979). "Kinetics of fluphenazine after fluphenazine dihydrochloride, enanthate and decanoate administration to man". Br J Clin Pharmacol. 7 (4): 325–31. doi:10.1111/j.1365-2125.1979.tb00941.x. PMC 1429660. PMID 444352.
- Young. D.: Ereshefsky. L.: Saklad. S.R.; Jann. M.W. and Garcia. N.: Explaining the pharmacokinetics of fluphenazine through computer simulations. (Abstract.) Presented at the 19th Annual Midyear Clinical Meeting of the American Society of Hospital Pharmacists. Dallas. Texas (1984).
- Janssen PA, Niemegeers CJ, Schellekens KH, Lenaerts FM, Verbruggen FJ, van Nueten JM, Marsboom RH, Hérin VV, Schaper WK (November 1970). "The pharmacology of fluspirilene (R 6218), a potent, long-acting and injectable neuroleptic drug". Arzneimittelforschung. 20 (11): 1689–98. PMID 4992598.
- Beresford R, Ward A (January 1987). "Haloperidol decanoate. A preliminary review of its pharmacodynamic and pharmacokinetic properties and therapeutic use in psychosis". Drugs. 33 (1): 31–49. doi:10.2165/00003495-198733010-00002. PMID 3545764.
- Reyntigens AJ, Heykants JJ, Woestenborghs RJ, Gelders YG, Aerts TJ (1982). "Pharmacokinetics of haloperidol decanoate. A 2-year follow-up". Int Pharmacopsychiatry. 17 (4): 238–46. doi:10.1159/000468580. PMID 7185768.
- Larsson, M., Axelsson, R., & Forsman, A. (1984). On the pharmacokinetics of perphenazine: a clinical study of perphenazine enanthate and decanoate. Current Therapeutic Research, 36(6), 1071–1088. https://scholar.google.com/scholar?cluster=12503004172250709786