Levonorgestrel butanoate
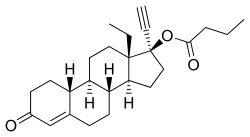
Levonorgestrel butanoate (LNG-B) (developmental code name HRP-002),[1][2] or levonorgestrel 17β-butanoate, is a steroidal progestin of the 19-nortestosterone group which was developed by the World Health Organization (WHO) in collaboration with the Contraceptive Development Branch (CDB) of the National Institute of Child Health and Human Development as a long-acting injectable contraceptive.[3][4][5] It is the C17β butanoate ester of levonorgestrel, and acts as a prodrug of levonorgestrel in the body.[4] The drug is at or beyond the phase III stage of clinical development, but has not been marketed at this time.[3] It was first described in the literature, by the WHO, in 1983, and has been under investigation for potential clinical use since then.[4][6]
 | |
| Clinical data | |
|---|---|
| Other names | LNG-B; HRP-002; Levonorgestrel 17β-butanoate; 17α-Ethynyl-18-methyl-19-nortestosterone 17β-butanoate; 17α-Ethynyl-18-methylestr-4-en-17β-ol-3-one 17β-butanoate |
| Routes of administration | Intramuscular injection |
| Drug class | Progestogen; Progestogen ester |
| ATC code |
|
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| ChemSpider | |
| UNII | |
| ECHA InfoCard | 100.081.125 |
| Chemical and physical data | |
| Formula | C25H34O3 |
| Molar mass | 382.544 g·mol−1 |
| 3D model (JSmol) | |
| |
| |
LNG-B has been under investigation as a long-lasting injectable contraceptive for women.[7] A single intramuscular injection of an aqueous suspension of 5 or 10 mg LNG-B has a duration of 3 months,[3][7] whereas an injection of 50 mg has a duration of 6 months.[1] The drug was also previously tested successfully as a combined injectable contraceptive with estradiol hexahydrobenzoate, but this formulation was never marketed.[7] LNG-B has been tested successfully in combination with testosterone buciclate as a long-lasting injectable contraceptive for men as well.[8][9]
LNG-B may have several advantages over depot medroxyprogesterone acetate, including the use of much lower comparative dosages, reduced progestogenic side effects like hypogonadism and amenorrhea, and a more rapid return in fertility following discontinuation.[7][10] The drug has a well-established safety record owing to the use of levonorgestrel as an oral contraceptive since the 1960s.[7]
| Progestogen | Form | Major brand names | Class | TFD (14 days) | POIC-D (2–3 months) | CIC-D (month) | Duration | |
|---|---|---|---|---|---|---|---|---|
| Algestone acetophenide | Oil solution | Perlutal, Topasel, Yectames | Pregnane | ? | – | 75–150 mg | 100 mg ≈ 14–32 days | |
| Cyproterone acetate | Oil solution | Androcur Depot | Pregnane | ? | – | – | 300 mg ≈ 20 days | |
| Dydrogesteronea | Aqueous suspension | – | Retropregnane | ? | – | – | 100 mg ≈ 16–38 days | |
| Gestonorone caproate | Oil solution | Depostat, Primostat | Norpregnane | 25–50 mg | – | – | 25–50 mg ≈ 8–13 days | |
| Hydroxyprogesterone acetatea | Aqueous suspension | – | Pregnane | 350 mg | – | – | 150–350 mg ≈ 9–16 days | |
| Hydroxyprogesterone caproate | Oil solution | Delalutin, Proluton, Makena | Pregnane | 250–500 mgb | – | 250–500 mg | 65–500 mg ≈ 5–21 days | |
| Levonorgestrel butanoatea | Aqueous suspension | – | Gonane | ? | – | – | 5–50 mg ≈ 3–6 months | |
| Lynestrenol phenylpropionatea | Oil solution | – | Estrane | ? | – | – | 50–100 mg ≈ 14–30 days | |
| Medroxyprogesterone acetate | Aqueous suspension | Depo-Provera | Pregnane | 50–100 mg | 150 mg | 25 mg | 50–150 mg ≈ 14–50+ days | |
| Megestrol acetate | Aqueous suspension | Mego-E | Pregnane | ? | – | 25 mg | 25 mg ≈ >14 daysc | |
| Norethisterone enanthate | Oil solution | Noristerat, Mesigyna | Estrane | 100–200 mg | 200 mg | 50 mg | 50–200 mg ≈ 11–52 days | |
| Oxogestone phenylpropionatea | Oil solution | – | Norpregnane | ? | – | – | 100 mg ≈ 19–20 days | |
| Progesterone | Oil solution | Progestaject, Gestone, Strone | Pregnane | 200 mgb | – | – | 25–350 mg ≈ 2–6 days | |
| Aqueous suspension | Agolutin Depot | Pregnane | 50–200 mg | – | – | 50–300 mg ≈ 7–14 days | ||
| Note: All by intramuscular or subcutaneous injection. All are synthetic except for P4, which is bioidentical. P4 production during the luteal phase is ~25 (15–50) mg/day. The OID of OHPC is 250 to 500 mg/month. Footnotes: a = Never marketed by this route. b = In divided doses (2 × 125 or 250 mg for OHPC, 10 × 20 mg for P4). c = Half-life is ~14 days. Sources: Main: See template. | ||||||||
See also
References
- King TL, Brucker MC, Kriebs JM, Fahey JO (21 October 2013). Varney's Midwifery. Jones & Bartlett Publishers. pp. 495–. ISBN 978-1-284-02542-2.
- Shalender Bhasin (13 February 1996). Pharmacology, Biology, and Clinical Applications of Androgens: Current Status and Future Prospects. John Wiley & Sons. pp. 401–. ISBN 978-0-471-13320-9.
- Benno Clemens Runnebaum; Thomas Rabe; Ludwig Kiesel (6 December 2012). Female Contraception: Update and Trends. Springer Science & Business Media. pp. 429–. ISBN 978-3-642-73790-9.
- Crabbé P, Archer S, Benagiano G, Diczfalusy E, Djerassi C, Fried J, Higuchi T (1983). "Long-acting contraceptive agents: design of the WHO Chemical Synthesis Programme". Steroids. 41 (3): 243–53. doi:10.1016/0039-128X(83)90095-8. PMID 6658872.
- Koetsawang S (1991). "The injectable contraceptive: present and future trends". Ann. N. Y. Acad. Sci. 626: 30–42. doi:10.1111/j.1749-6632.1991.tb37897.x. PMID 1829341.
- Benagiano, G., & Merialdi, M. (2011). Carl Djerassi and the World Health Organisation special programme of research in human reproduction. Journal für Reproduktionsmedizin und Endokrinologie-Journal of Reproductive Medicine and Endocrinology, 8(1), 10-13. http://www.kup.at/kup/pdf/10163.pdf
- Paolo Giovanni Artini; Andrea R. Genazzani; Felice Petraglia (11 December 2001). Advances in Gynecological Endocrinology. CRC Press. pp. 105–. ISBN 978-1-84214-071-0.
- C. Coutifaris; L. Mastroianni (15 August 1997). New Horizons in Reproductive Medicine. CRC Press. pp. 101–. ISBN 978-1-85070-793-6.
- Shio Kumar Singh (4 September 2015). Mammalian Endocrinology and Male Reproductive Biology. CRC Press. pp. 270–. ISBN 978-1-4987-2736-5.
- Pramilla Senanayake; Malcolm Potts (14 April 2008). Atlas of Contraception, Second Edition. CRC Press. pp. 49–. ISBN 978-0-203-34732-4.