Iodine deficiency
Iodine deficiency is a lack of the trace element iodine, an essential nutrient in the diet. It may result in metabolic problems such as goiter, sometimes as an endemic goiter as well as cretinism due to untreated congenital hypothyroidism, which results in developmental delays and other health problems. Iodine deficiency is an important global health issue, especially for fertile and pregnant women. It is also a preventable cause of intellectual disability.
| Iodine deficiency | |
|---|---|
| Specialty | Endocrinology |
Iodine is an essential dietary mineral for neurodevelopment among offsprings and toddlers.[1] The thyroid hormones thyroxine and triiodothyronine contain iodine. In areas where there is little iodine in the diet, typically remote inland areas where no marine foods are eaten, iodine deficiency is common. It is also common in mountainous regions of the world where food is grown in iodine-poor soil.
Prevention includes adding small amounts of iodine to table salt, a product known as iodized salt. Iodine compounds have also been added to other foodstuffs, such as flour, water and milk, in areas of deficiency.[2] Seafood is also a well known source of iodine.[3]
In the U.S., the use of iodine has decreased over concerns of overdoses since mid-20th century, and the iodine antagonists bromine, perchlorate and fluoride have become more ubiquitous.[4] In particular, around 1980 the practice of using potassium iodate as dough conditioner in bread and baked goods was gradually replaced by the use of other conditioning agents[5] such as bromide.
Iodine deficiency resulting in goiter occurs in 187 million people globally as of 2010 (2.7% of the population).[6] It resulted in 2700 deaths in 2013 up from 2100 deaths in 1990.[7]
Signs and symptoms
Goiter
A low amount of thyroxine (one of the two thyroid hormones) in the blood, due to lack of dietary iodine to make it, gives rise to high levels of thyroid stimulating hormone (TSH), which stimulates the thyroid gland to increase many biochemical processes; the cellular growth and proliferation can result in the characteristic swelling or hyperplasia of the thyroid gland, or goiter. In mild iodine deficiency, levels of triiodothyronine (T3) may be elevated in the presence of low levels of levothyroxine, as the body converts more of the levothyroxine to triiodothyronine as a compensation. Some such patients may have a goiter, without an elevated TSH. The introduction of iodized salt since the early 1900s has eliminated this condition in many affluent countries; however, in Australia, New Zealand, and several European countries, iodine deficiency is a significant public health problem.[8] It is more common in developing countries. Public health initiatives to lower the risk of cardiovascular disease have resulted in lower discretionary salt use at the table. Additionally, there is a trend towards consuming more processed foods in western countries. The noniodized salt used in these foods means that people are less likely to obtain iodine from adding salt during cooking.
Goiter is said to be endemic when the prevalence in a population is > 5%, and in most cases goiter can be treated with iodine supplementation. If goiter is untreated for around five years, however, iodine supplementation or thyroxine treatment may not reduce the size of the thyroid gland because the thyroid is permanently damaged.
Congenital iodine deficiency syndrome
Congenital iodine deficiency syndrome, previously known as cretinism, is a condition associated with iodine deficiency and goiter, commonly characterised by mental deficiency, deafness, squint, disorders of stance and gait and stunted growth due to hypothyroidism. Paracelsus was the first to point out the relation between goitrous parents and their mentally disabled children.[9]
As a result of restricted diet, isolation, intermarriage, etc., as well as low iodine content in their food, children often had peculiar stunted bodies and retarded mental faculties, a condition later known to be associated with thyroid hormone deficiency. Diderot, in his 1754 Encyclopédie, described these patients as "crétins". In French, the term "crétin des Alpes" also became current, since the condition was observed in remote valleys of the Alps in particular. The word cretin appeared in English in 1779.
While reporting recent progress towards overcoming iodine-deficiency disorders worldwide, The Lancet noted: "According to World Health Organization, in 2007, nearly 2 billion individuals had insufficient iodine intake, a third being of school age." A conclusion was made that the single most preventable cause of intellectual disability is that of iodine deficiency.[10]
Fibrocystic breast changes
There is preliminary evidence that iodine deficiency enhances the sensitivity of breast tissue to estrogen.[11][12] In rats treated with estradiol, iodine deficiency has been shown to lead to changes similar to benign breast changes that are reversible by increased iodine in the diet.[11][12] In a few studies, iodine supplementation had beneficial effects (such as reducing the presence of breast cyst, fibrous tissue plaques and breast pain) in women with fibrocystic breast changes.[11][13]
Protective effects of iodine on breast cancer have been postulated from epidemiologic evidence and described in animal models.[14][15][16] In view of the antiproliferative properties of iodine in breast tissue, molecular iodine supplementation has been suggested as an adjuvant in breast cancer therapy.[16]
Risk factors
Following is a list of potential risk factors that may lead to iodine deficiency:[17]
- Low dietary iodine
- Selenium deficiency
- Pregnancy
- Exposure to radiation
- Increased intake/plasma levels of goitrogens, such as calcium
- Sex (higher occurrence in women)
- Smoking tobacco
- Alcohol (reduced prevalence in users)
- Oral contraceptives (reduced prevalence in users)
- Perchlorates
- Thiocyanates
- Age (for different types of iodine deficiency at different ages)
Pathophysiology
Iodine accounts for 65% of the molecular weight of T4 and 59% of T3. There is a total of 15–20 mg of iodine in the human body, primarily concentrated in thyroid tissue and hormones. Thirty percent of iodine is distributed in other tissues, including the mammary glands, eyes, gastric mucosa, choroid plexus, arterial walls, the cervix, and salivary glands. In the cells of these tissues, iodide enters directly by sodium-iodide symporter (NIS).
- Venturi S, Guidi A, Venturi M (1996). "[Extrathyroid iodine deficiency disorders: what is the real iodine requirement?]"". Le Basi Razionali della Terapia. 16: 267–275.
- Pellerin P (1961). "La tecnique d'autoradiographie anatomique a la temperature de l'azote liquide". Path Biol. 232 (9): 233–252.
Diagnosis

The diagnostic workup of a suspected iodine deficiency includes signs and symptoms as well as possible risk factors mentioned above. A 24-hour urine iodine collection is a useful medical test, as approximately 90% of ingested iodine is excreted in the urine.[19] For the standardized 24-hour test, a 50 mg iodine load is given first, and 90% of this load is expected to be recovered in the urine of the following 24 hours. Recovery of less than 90% is taken to mean high retention, that is, iodine deficiency. The recovery may, however, be well less than 90% during pregnancy, and an intake of goitrogens can alter the test results.[20]
If a 24-hour urine collection is not practical, a random urine iodine-to-creatinine ratio can alternatively be used.[19] However, the 24-hour test is found to be more reliable.[21]
A general idea of whether a deficiency exists can be determined through a functional iodine test in the form of an iodine skin test. In this test, the skin is painted with an iodine solution: if the iodine patch disappears quickly, this is taken as a sign of iodine deficiency. However, no accepted norms exist on the expected time interval for the patch to disappear, and in persons with dark skin color the disappeance of the patch may be difficult to assess. If a urine test is taken shortly after, the results may be altered due to the iodine absorbed previously in a skin test.[20]
Treatment

Iodine deficiency is treated by ingestion of iodine salts, such as found in food supplements. Mild cases may be treated by using iodized salt in daily food consumption, or drinking more milk, or eating egg yolks, and saltwater fish. For a salt and/or animal product restricted diet, sea vegetables (kelp, hijiki, dulse, nori (found in sushi)) may be incorporated regularly into a diet as a good source of iodine.[19]
The recommended daily intake of iodine for adult women is 150–300 µg for maintenance of normal thyroid function; for men, it is somewhat less at 150 µg.[19]
Nonetheless, there is a lack of evidence on iodine fortification in foods, beverages, condiments, or seasonings other than salt in preventing goiter or improving physical development. On the other hand, such a measure may increase iodine concentration in urine.[22]
However, too high iodine intake, for example due to overdosage of iodine supplements, can have toxic side effects. It can lead to hyperthyroidism and consequently high blood levels of thyroid hormones (hyperthyroxinemia). In case of extremely high single-dose iodine intake, typically a short-term suppression of thyroid function (Wolff–Chaikoff effect) occurs.[23] Persons with pre-existing thyroid disease, elderly persons, fetuses and neonates, and patients with other risk factors are at a higher risk of experiencing iodine-induced thyroid abnormalities.[24] In particular, in persons with goiter due to iodine deficiency or with altered thyroid function, a form of hyperthyroidism called Jod-Basedow phenomenon can be triggered even at small or single iodine dosages, for example as a side effect of administration of iodine-containing contrast agents. In some cases, excessive iodine contributes to a risk of autoimmune thyroid diseases (Hashimoto's thyroiditis[25] and Graves' disease[26]).
Prognosis
With iodine supplementation, goiters caused by iodine deficiency decrease in size in very young children and pregnant women. Generally, however, long-standing goiters caused by iodine deficiency respond with only small amounts of shrinkage after iodine supplementation, and patients are at risk for developing hyperthyroidism.[19] Following the adoption of iodised salt in the United States in 1924, there was a gradual increase in average intelligence of 1 standard deviation, 15 points in iodine-deficient areas, 3.5 points nationally, but also an increase in deaths of older people in iodine-deficient areas due to hyperthyroidism.[27]
Epidemiology
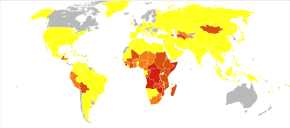
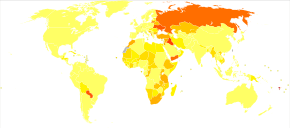
Iodine deficiency resulting in goiter occurs in 187 million people globally as of 2010 (2.7% of the population).[6] Certain areas of the world, due to natural deficiency and unavailability of iodine, are severely affected by iodine deficiency, which affects approximately two billion people worldwide. It is particularly common in the Western Pacific, South-East Asia and Africa. Among other nations affected by iodine deficiency, China and Kazakhstan have begun taking action, while Russia has not. Successful campaigns for the adoption of the use of iodized salt require education of salt producers and sellers and a communication campaign directed at the public. The cost of adding iodine to salt is negligible—"Only a few cents a ton."[29]
Iodine deficiency has largely been confined to the developing world for several generations, but reductions in salt consumption and changes in dairy processing practices eliminating the use of iodine-based disinfectants have led to increasing prevalence of the condition in Australia and New Zealand in recent years. A proposal to mandate the use of iodized salt in most commercial breadmaking was adopted there in October, 2009.[30] In a study of the United Kingdom published in 2011, almost 70% of test subjects were found to be iodine deficient.[31] The study's authors suggested an investigation regarding "evidence-based recommendations for iodine supplementation".[31]
It is well known that micronutrient deficiencies change the development of intelligence and iodine is no exception. Lacking iodine during human development causes a fall, in average, of 12 IQ points in China.[32] It has been found in the U.S. that the proliferation of iodized salt increased IQ by 15 points in some areas.[33]
In iodine-deficient or mildly iodine-deficient areas of Europe, iodine deficiency is frequent during pregnancy despite the widespread use of iodised salt, posing risks to the neurodevelopment of foetuses.[34] In one study performed in a mildly iodine-deficient area, iodine deficiency was found to be present in more than half of breastfeeding women; in contrast, the majority of their newborns had iodine excess, mostly due to neonatal exposure to iodine-containing disinfectants.[35] A 2014 meta-analysis found that iodine supplementation "improves some maternal thyroid indices and may benefit aspects of cognitive function in school-age children, even in marginally iodine-deficient areas."[36]
Deficient populations
In areas where there is little iodine in the diet, typically remote inland areas and semi-arid equatorial climates where no marine foods are eaten, iodine deficiency gives rise to hypothyroidism, symptoms of which are extreme fatigue, goiter, mental slowing, depression, weight gain, and low basal body temperatures.[37]
Iodine deficiency is the leading cause of preventable mental retardation, a result which occurs primarily when babies or small children are rendered hypothyroidic by a lack of the element. The addition of iodine to table salt has largely eliminated this problem in the wealthier nations, but as of March 2006, iodine deficiency remained a serious public health problem in the developing world.[38]
Iodine deficiency is also a problem in certain areas of Europe. In Germany it has been estimated to cause a billion dollars in health care costs per year.[13] A modelling analysis suggests universal iodine supplementation for pregnant women in England may save £199 (2013 UK pounds) to the health service per pregnant woman and save £4476 per pregnant woman in societal costs.[39]
Iodine deficiency was previously a common disease in Norway, because the content of iodine in the drinking water was low. Before 1950 goiter was a widespread disease caused by iodine deficiency.[40] Up to 80 per cent of the population were affected in inland areas. In the coastal communities, saltwater fish were an important part of the diet, and because of the presence of iodine in seawater, goiter was less common than in the inland districts. From the 1950s, Norwegians started adding iodine to dairy cow feed. Since milk was an essential part of the Norwegian diet, the incidence of goiter decreased in the population.[40]
See also
- Basil Hetzel
- Lugol's iodine
- International Council for the Control of Iodine Deficiency Disorders
References
- "Risiko For Jodmangel i Norge" (PDF). Ernæringsrådet (in Norwegian). June 2016.
- Creswell J. Eastman; Michael Zimmermann (12 February 2014). "The Iodine Deficiency Disorders". Thyroid Disease Manager. Retrieved 2016-12-11.
- "Iodine in Seaweed". Archived from the original on 2012-07-31. Retrieved 2008-01-04.
- Meletis, C. D. (2011). "Iodine: Health Implications of Deficiency". Journal of Evidence-Based Complementary & Alternative Medicine. 16 (3): 190–194. doi:10.1177/2156587211414424. ISSN 1533-2101.
- K. Smith (24 August 1988). Trace Minerals in Foods. CRC Press. pp. 273–. ISBN 978-0-8247-7835-4.
- Vos, T; Flaxman, A. D.; Naghavi, M; Lozano, R; Michaud, C; Ezzati, M; Shibuya, K; Salomon, J. A.; Abdalla, S; Aboyans, V; Abraham, J; Ackerman, I; Aggarwal, R; Ahn, S. Y.; Ali, M. K.; Alvarado, M; Anderson, H. R.; Anderson, L. M.; Andrews, K. G.; Atkinson, C; Baddour, L. M.; Bahalim, A. N.; Barker-Collo, S; Barrero, L. H.; Bartels, D. H.; Basáñez, M. G.; Baxter, A; Bell, M. L.; Benjamin, E. J.; et al. (Dec 15, 2012). "Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010". Lancet. 380 (9859): 2163–96. doi:10.1016/S0140-6736(12)61729-2. PMC 6350784. PMID 23245607.
- GBD 2013 Mortality and Causes of Death, Collaborators (17 December 2014). "Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013". Lancet. 385 (9963): 117–171. doi:10.1016/S0140-6736(14)61682-2. PMC 4340604. PMID 25530442.
- Andersson M, Takkouche B, Egli I, Allen HE, de Benoist B (2005). "Current global iodine status and progress over the last decade towards the elimination of iodine deficiency". Bull. World Health Organ. 83 (7): 518–25. PMC 2626287. PMID 16175826.
- T.E.C., Jr. (August 1, 1974). "Paracelsus on What the Physician Should Know". Pediatrics. American Academy of Pediatrics. 54 (2). Retrieved 2008-12-05.
- The Lancet (12 July 2008). "Iodine deficiency—way to go yet". The Lancet. 372 (9633): 88. doi:10.1016/S0140-6736(08)61009-0. PMID 18620930. Retrieved 2008-12-05.
- Cann, Stephen A.; van Netten, Johannes P.; van Netten, Christiaan (2000). "Hypothesis: iodine, selenium and the development of breast cancer". Cancer Causes and Control (review). 11 (2): 121–127. doi:10.1023/A:1008925301459. ISSN 0957-5243. PMID 10710195.
- Joseph E. Pizzorno; Michael T. Murray (14 September 2012). Textbook of Natural Medicine. Elsevier Health Sciences. p. 1371. ISBN 978-1-4377-2333-5.
- Patrick L (2008). "Iodine: deficiency and therapeutic considerations". Altern Med Rev. 13 (2): 116–27. PMID 18590348.
- "Iodine Monograph" (PDF). Alternative Medicine Review. 15 (3): 273–278. 2010.
- Venturi S (October 2001). "Is there a role for iodine in breast diseases?". Breast. 10 (5): 379–82. doi:10.1054/brst.2000.0267. PMID 14965610.
- Aceves C, Anguiano B, Delgado G (April 2005). "Is iodine a gatekeeper of the integrity of the mammary gland?". Journal of Mammary Gland Biology and Neoplasia (review). 10 (2): 189–96. doi:10.1007/s10911-005-5401-5. PMID 16025225.
- Knudsen N, Laurberg P, Perrild H, Bülow I, Ovesen L, Jørgensen T (October 2002). "Risk factors for goiter and thyroid nodules". Thyroid. 12 (10): 879–88. doi:10.1089/105072502761016502. PMID 12487770.
- Venturi, S.; Donati, F.M.; Venturi, A.; Venturi, M. (2000). "Environmental Iodine Deficiency: A Challenge to the Evolution of Terrestrial Life?". Thyroid. 10 (8): 727–9. doi:10.1089/10507250050137851. PMID 11014322.
- Stephanie L. Lee; Elizabeth N. Pearce; Sonia Ananthakrishnan (16 December 2015). "Iodine Deficiency". Medscape. Retrieved 2016-12-11.
- Richard S. Lord; J. Alexander Bralley (2008). Laboratory Evaluations for Integrative and Functional Medicine. Metametrix Institute. pp. 107–108. ISBN 978-0-9673949-4-7.
- Richard S. Lord; J. Alexander Bralley (2008). Laboratory Evaluations for Integrative and Functional Medicine. Metametrix Institute. p. 106. ISBN 978-0-9673949-4-7.
- Alvin-R-Santos,J, Christoforou A, Trieu K, McKenzie BL, Downs S, Billot L, Webster J, Li M (12 February 2019). "Iodine Fortification of Foods and Condiments, Other Than Salt, for Preventing Iodine Deficiency Disorders". Cochrane Database of Systematic Reviews (2): CD010734. doi:10.1002/14651858.CD010734.pub2. PMC 6370918. PMID 30746700.CS1 maint: multiple names: authors list (link)
- Sabyasachi Sircar (2008). Principles of Medical Physiology. Thieme. p. 513. ISBN 978-1-58890-572-7.
- Leung, Angela M.; Braverman, Lewis E. (2013). "Consequences of excess iodine". Nature Reviews Endocrinology. 10 (3): 136–142. doi:10.1038/nrendo.2013.251. ISSN 1759-5029. PMC 3976240. PMID 24342882.
- Rose NR, Bonita R, Burek CL (February 2002). "Iodine: an environmental trigger of thyroiditis". Autoimmunity Reviews. 1 (1–2): 97–103. CiteSeerX 10.1.1.326.5700. doi:10.1016/s1568-9972(01)00016-7. PMID 12849065.
- Laurberg, P.; Pedersen, K. M.; Vestergaard, H.; Sigurdsson, G. (1991). "High incidence of multinodular toxic goitre in the elderly population in a low iodine intake area vs. high incidence of Graves' disease in the young in a high iodine intake area: comparative surveys of thyrotoxicosis epidemiology in East-Jutland Denmark and Iceland". Journal of Internal Medicine. 229 (5): 415–420. doi:10.1111/j.1365-2796.1991.tb00368.x. ISSN 0954-6820. PMID 2040867.
- Max Nisen (July 22, 2013). "How Adding Iodine To Salt Resulted In A Decade's Worth Of IQ Gains For The United States". Business Insider. Retrieved July 23, 2013.
- "Mortality and Burden of Disease Estimates for WHO Member States in 2002" (xls). World Health Organization. 2002.
- "In Raising the World's I.Q., the Secret's in the Salt", article by Donald G. McNeil, Jr., The New York Times, December 16, 2006.
- l "Iodine Fortification" Archived 2013-04-10 at the Wayback Machine, article appearing on March 5, 2013, from Food Standards.
- Vanderpump, M. P.; Lazarus, J. H.; Smyth, P. P.; Laurberg, P; Holder, R. L.; Boelaert, K; Franklyn, J. A.; British Thyroid Association UK Iodine Survey Group (11 June 2011). "Iodine status of UK schoolgirls: a cross-sectional survey". The Lancet. 377 (9782): 2007–12. doi:10.1016/S0140-6736(11)60693-4. PMID 21640375.
- Qian M, Wang D, Watkins WE, et al. (2005). "The effects of iodine on intelligence in children: a meta-analysis of studies conducted in China". Asia Pacific Journal of Clinical Nutrition. 14 (1): 32–42. PMID 15734706.
- "How Adding Iodine to Salt Resulted in a Decade's Worth of IQ Gains for the United States".
- Trumpff, Caroline; De Schepper, Jean; Tafforeau, Jean; Van Oyen, Herman; Vanderfaeillie, Johan; Vandevijvere, Stefanie (2013). "Mild iodine deficiency in pregnancy in Europe and its consequences for cognitive and psychomotor development of children: A review" (PDF). Journal of Trace Elements in Medicine and Biology. 27 (3): 174–183. doi:10.1016/j.jtemb.2013.01.002. PMID 23395294.
- Yaman AK, Demirel F, Ermiş B, Pişkin IE (2013). "Maternal and neonatal urinary iodine status and its effect on neonatal TSH levels in a mildly iodine-deficient area". Journal of Clinical Research in Pediatric Endocrinology. 5 (2): 90–4. doi:10.4274/Jcrpe.997. PMC 3701928. PMID 23748060.
- Taylor PN, Okosieme OE, Dayan CM, Lazarus JH (January 2014). "Therapy of endocrine disease: Impact of iodine supplementation in mild-to-moderate iodine deficiency: systematic review and meta-analysis". European Journal of Endocrinology (review). 170 (1): R1–R15. doi:10.1530/EJE-13-0651. PMID 24088547.
- Felig, Philip; Frohman, Lawrence A. (2001). "Endemic Goiter". Endocrinology & metabolism. McGraw-Hill Professional. ISBN 978-0-07-022001-0.
- "Micronutrients — Iodine, Iron and Vitamin A". UNICEF.
- Monahan, Mark; Boelaert, Kristien; Jolly, Kate; Chan, Shiao; Barton, Pelham; Roberts, Tracy E (2015-01-01). "Costs and benefits of iodine supplementation for pregnant women in a mildly to moderately iodine-deficient population: a modelling analysis" (PDF). The Lancet Diabetes & Endocrinology. 3 (9): 715–722. doi:10.1016/s2213-8587(15)00212-0. PMID 26268911.
- "Fakta om jod" [Facts about iodine]. Folkehelseinstituttet (in Norwegian). Retrieved 2018-07-11.
Further reading
- Kotwal A, Priya R, Qadeer I (2007). "Goiter and other iodine deficiency disorders: A systematic review of epidemiological studies to deconstruct the complex web". Arch. Med. Res. 38 (1): 1–14. doi:10.1016/j.arcmed.2006.08.006. PMID 17174717.
External links
| Classification |
|
|---|---|
| External resources |
| Authority control |
|
|---|