Hyperparathyroidism
Hyperparathyroidism is an increase in parathyroid hormone (PTH) levels in the blood.[1][4] This occurs from a disorder either within the parathyroid glands (primary hyperparathyroidism) or outside the parathyroid glands (secondary hyperparathyroidism).[1] Most people with primary disease have no symptoms at the time of diagnosis.[3] When symptoms occur, they are due to elevated blood calcium.[1] With long-standing elevation, the most common symptom is kidney stones.[1] Other symptoms may include bone pain, weakness, depression, confusion, and increased urination.[1][2] Both primary and secondary may result in osteoporosis (weakening of the bones).[2][3]
| Hyperparathyroidism | |
|---|---|
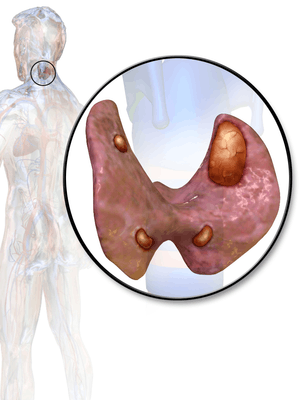
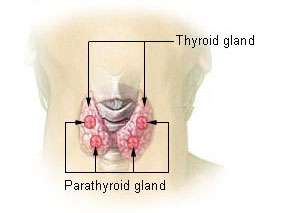 | |
| Thyroid and parathyroid | |
| Specialty | Endocrinology |
| Symptoms | None, kidney stones, weakness, depression, bone pains, confusion, increased urination[1][2][3] |
| Complications | Osteoporosis[2][3] |
| Usual onset | 50 to 60[2] |
| Types | Primary, secondary |
| Causes | Primary: parathyroid adenoma, multiple benign tumors, parathyroid cancer[1][2] Secondary: vitamin D deficiency, chronic kidney disease, low blood calcium[1] |
| Diagnostic method | High blood calcium and high PTH levels[2] |
| Treatment | Monitoring, surgery, intravenous normal saline, cinacalcet[1][2] |
| Frequency | ~2 per 1,000[3] |
In 80% of cases, primary hyperparathyroidism is due to a single benign tumor known as a parathyroid adenoma.[1][2] Most of the remainder are due to several of these adenomas.[1][2] Rarely it may be due to parathyroid cancer.[2] Secondary hyperparathyroidism typically occurs due to vitamin D deficiency, chronic kidney disease, or other causes of low blood calcium.[1] The diagnosis of primary hyperparathyroidism is made by finding elevated calcium and PTH in the blood.[2]
Primary hyperparathyroidism may be cured by removing the adenoma or overactive parathyroid glands.[1][2] In those without symptoms, mildly increased blood calcium levels, normal kidneys, and normal bone density monitoring may be all that is required.[2] The medication cinacalcet may also be used to decrease PTH levels.[2] In those with very high blood calcium levels, treatment may include large amounts of intravenous normal saline.[1] Low vitamin D levels should be corrected.[2]
Primary hyperparathyroidism is the most common type.[1] In the developed world, between one and four per thousand people are affected.[3] It occurs three times more often in women than men and is typically diagnosed between the ages of 50 and 60.[2] The disease was first described in the 1700s.[5] In the late 1800s, it was determined to be related to the parathyroid.[5] Surgery as a treatment was first carried out in 1925.[5]
Signs and symptoms
Symptoms depend on whether the hyperparathyroidism is the result of parathyroid overactivity or secondary.
In primary hyperparathyroidism, about 75% of people have no symptoms.[1] The problem is often picked up incidentally during blood work for other reasons, and the test results show a higher amount of calcium in the blood than normal.[3] Many other people only have non-specific symptoms.
Symptoms directly due to hypercalcemia are relatively rare, being more common in patients with malignant hypercalcemia. If present, common manifestations of hypercalcemia include weakness and fatigue, depression, bone pain, muscle soreness (myalgias), decreased appetite, feelings of nausea and vomiting, constipation, polyuria, polydipsia, cognitive impairment, kidney stones ([nb 1]) and osteopenia or osteoporosis.[8] A history of acquired racquet nails (brachyonychia) may be indicative of bone resorption.[9] Parathyroid adenomas are very rarely detectable on clinical examination. Surgical removal of a parathyroid tumor eliminates the symptoms in most patients.
In secondary hyperparathyroidism, the parathyroid gland is behaving normally; clinical problems are due to bone resorption and manifest as bone syndromes such as rickets, osteomalacia, and renal osteodystrophy.
Causes
Radiation exposure increases the risk of primary hyperparathyroidism.[1] A number of genetic conditions including multiple endocrine neoplasia syndromes also increase the risk.[1]
Mechanism
Normal parathyroid glands measure the ionized calcium (Ca2+) concentration in the blood and secrete parathyroid hormone accordingly; if the ionized calcium rises above normal, the secretion of PTH is decreased, whereas when the Ca2+ level falls, parathyroid hormone secretion is increased.[6]
Secondary hyperparathyroidism occurs if the calcium level is abnormally low. The normal glands respond by secreting parathyroid hormone at a persistently high rate. This typically occurs when the 1,25 dihydroxyvitamin D3 levels in the blood are low and hypocalcemia is present. A lack of 1,25 dihydroxyvitamin D3 can result from a deficient dietary intake of vitamin D, or from a lack of exposure of the skin to sunlight, so the body cannot make its own vitamin D from cholesterol.[10] The resulting hypovitaminosis D is usually due to a partial combination of both factors. Vitamin D3 (or cholecalciferol) is converted to 25-hydroxyvitamin D (or calcidiol) by the liver, from where it is transported via the circulation to the kidneys, and it is converted into the active hormone, 1,25 dihydroxyvitamin D3.[6][10] Thus, a third cause of secondary hyperparathyroidism is chronic kidney disease. Here the ability to manufacture 1,25 dihydroxyvitamin D3 is compromised, resulting in hypocalcemia.
Diagnosis


The gold standard of diagnosis is the PTH immunoassay. Once an elevated PTH has been confirmed, the goal of diagnosis is to determine whether the hyperparathyroidism is primary or secondary in origin by obtaining a serum calcium level:
| Serum calcium | Phosphate | ALP | PTH | Likely type |
| ↑ | ↓ | ↑ | ↑ | Primary hyperparathyroidism[11] |
| ↓ | ↑ | ↑ | ↑ | Secondary hyperparathyroidism[11] |
Tertiary hyperparathyroidism has a high PTH and a high serum calcium. It is differentiated from primary hyperparathyroidism by a history of chronic kidney failure and secondary hyperparathyroidism.
Hyperparathyroidism can cause hyperchloremia and increase renal bicarbonate loss, which may result in a normal anion gap metabolic acidosis.[5]
Differential diagnosis
Familial benign hypocalciuric hypercalcaemia can present with similar lab changes.[1] In this condition, the calcium creatinine clearance ratio, however, is typically under 0.01.[1]
Blood tests
Intact PTH
In primary hyperparathyroidism, parathyroid hormone (PTH) levels are either elevated or "inappropriately normal" in the presence of elevated calcium. Typically, PTH levels vary greatly over time in the affected patient and (as with Ca and Ca++ levels) must be retested several times to see the pattern. The currently accepted test for PTH is intact PTH, which detects only relatively intact and biologically active PTH molecules. Older tests often detected other, inactive fragments. Even intact PTH may be inaccurate in patients with kidney dysfunction.
Calcium levels
In cases of primary hyperparathyroidism or tertiary hyperparathyroidism, heightened PTH leads to increased serum calcium (hypercalcemia) due to:
- increased bone resorption, allowing flow of calcium from bone to blood
- reduced kidney clearance of calcium
- increased intestinal calcium absorption
Serum phosphate
In primary hyperparathyroidism, serum phosphate levels are abnormally low as a result of decreased reabsorption of phosphate in the kidney tubules. However, this is only present in about 50% of cases. This contrasts with secondary hyperparathyroidism, in which serum phosphate levels are generally elevated because of kidney disease.
Alkaline phosphatase
Alkaline phosphatase levels are usually elevated in hyperparathyroidism. In primary hyperparathyroidism, levels may remain within the normal range, but this is inappropriately normal given the increased levels of plasma calcium.
Nuclear medicine
A technetium sestamibi scan is a procedure in nuclear medicine that identifies hyperparathyroidism (or parathyroid adenoma).[12] It is used by surgeons to locate ectopic parathyroid adenomas, most commonly found in the anterior mediastinum.
Classification
Primary
Primary hyperparathyroidism results from a hyperfunction of the parathyroid glands themselves. The oversecretion of PTH is due to a parathyroid adenoma, parathyroid hyperplasia, or rarely, a parathyroid carcinoma. This disease is often characterized by the quartet stones, bones, groans, and psychiatric overtones referring to the presence of kidney stones, hypercalcemia, constipation, and peptic ulcers, as well as depression, respectively.[13][14]
In a minority of cases, this occurs as part of a multiple endocrine neoplasia (MEN) syndrome, either type 1 (caused by a mutation in the gene MEN1) or type 2a (caused by a mutation in the gene RET). Other mutations that have been linked to parathyroid neoplasia include mutations in the genes HRPT2 and CASR.[15][16]
Patients with bipolar disorder who are receiving long-term lithium treatment are at increased risk for hyperparathyroidism.[17] Elevated calcium levels are found in 15% to 20% of patients who have been taking lithium long-term. However, only a few of these patients have significantly elevated levels of parathyroid hormone and clinical symptoms of hyperparathyroidism. Lithium-associated hyperparathyroidism is usually caused by a single parathyroid adenoma.[17]
Secondary
Secondary hyperparathyroidism is due to physiological (i.e. appropriate) secretion of parathyroid hormone (PTH) by the parathyroid glands in response to hypocalcemia (low blood calcium levels). The most common causes are vitamin D deficiency[18] (caused by lack of sunlight, diet or malabsorption) and chronic kidney failure.
Lack of vitamin D leads to reduced calcium absorption by the intestine leading to hypocalcemia and increased parathyroid hormone secretion. This increases bone resorption. In chronic kidney failure the problem is more specifically failure to convert vitamin D to its active form in the kidney. The bone disease in secondary hyperparathyroidism caused by kidney failure is termed renal osteodystrophy.
Tertiary
Tertiary hyperparathyroidism is seen in those with long-term secondary hyperparathyroidism, which eventually leads to hyperplasia of the parathyroid glands and a loss of response to serum calcium levels. This disorder is most often seen in patients with end-stage kidney disease and is an autonomous activity.
Treatment
Treatment depends on the type of hyperparathyroidism encountered.
Primary
People with primary hyperparathyroidism who are symptomatic benefit from parathyroidectomy—surgery to remove the parathyroid tumor (parathyroid adenoma). Indications for surgery are:[19]
- Symptomatic hyperparathyroidism
- Asymptomatic hyperparathyroidism with any of the following:
Surgery can rarely result in hypoparathyroidism.
Secondary
In people with secondary hyperparathyroidism, the high PTH levels are an appropriate response to low calcium and treatment must be directed at the underlying cause of this (usually vitamin D deficiency or chronic kidney failure). If this is successful, PTH levels return to normal levels, unless PTH secretion has become autonomous (tertiary hyperparathyroidism).
Calcimimetics
A calcimimetic (such as cinacalcet) is a potential therapy for some people with severe hypercalcemia and primary hyperparathyroidism who are unable to undergo parathyroidectomy, and for secondary hyperparathyroidism on dialysis.[20][21]
Treatment of secondary hyperparathyroidism with a calcimimetic in those on dialysis for CKD does not alter the risk of early death; however, it does decrease the likelihood of needing a parathyroidectomy.[22] Treatment carries the risk of low blood calcium levels and vomiting.[22]
History
The oldest known case was found in a cadaver from an Early Neolithic cemetery in southwest Germany.[23]
Notes
- Although parathyroid hormone (PTH) promotes the reabsorption of calcium from the kidneys' tubular fluid, thus decreasing the rate of urinary calcium excretion, its effect is only noticeable at any given plasma ionized calcium concentration. The primary determinant of the amount of calcium excreted into the urine per day is the plasma ionized calcium concentration. Thus, in primary hyperparathyroidism, the quantity of calcium excreted in the urine per day is increased despite the high levels of PTH in the blood, because hyperparathyroidism results in hypercalcemia, which increases the urinary calcium concentration (hypercalcuria). Kidney stones are, therefore, often a first indication of hyperparathyroidism, especially since the hypercalcuria is accompanied by an increase in urinary phosphate excretion (a direct result of the high plasma PTH levels). Together, the calcium and phosphate tend to precipitate out as water-insoluble salts, which readily form solid “stones”.[6][7]
References
- Fraser WD (July 2009). "Hyperparathyroidism". Lancet. 374 (9684): 145–58. doi:10.1016/S0140-6736(09)60507-9. PMID 19595349.
- "Primary Hyperparathyroidism". NIDDK. August 2012. Archived from the original on 4 October 2016. Retrieved 27 September 2016.
- Michels, TC; Kelly, KM (15 August 2013). "Parathyroid disorders". American Family Physician. 88 (4): 249–57. PMID 23944728.
- Allerheiligen, DA; Schoeber, J; Houston, RE; Mohl, VK; Wildman, KM (15 April 1998). "Hyperparathyroidism". American Family Physician. 57 (8): 1795–802, 1807–8. PMID 9575320.
- Gasparri, Guido; Camandona, Michele; Palestini, Nicola (2015). Primary, Secondary and Tertiary Hyperparathyroidism: Diagnostic and Therapeutic Updates. Springer. ISBN 9788847057586. Archived from the original on 2017-09-08.
- Blaine J, Chonchol M, Levi M (2015). "Renal control of calcium, phosphate, and magnesium homeostasis". Clinical Journal of the American Society of Nephrology. 10 (7): 1257–72. doi:10.2215/CJN.09750913. PMC 4491294. PMID 25287933.
- Harrison, T.R.; Adams, R.D.; Bennett Jnr., I.L.; Resnick, W.H.; Thorn, G.W.; Wintrobe, M.M. (1958). "Metabolic and Endocrine Disorders.". In: Principles of Internal Medicine (Third ed.). New York: McGraw-Hill Book Company. pp. 575–578.
- Hyperparathyroidism Archived 2011-05-24 at the Wayback Machine. National Endocrine and Metabolic Diseases Information Service. May 2006.
- Baran, R.; Turkmani, M.G.; Mubki, T. (2014). "Acquired Racquet Nails: a Useful Sign of Hyperparathyroidism". Journal of the European Academy of Dermatology and Venereology. 28 (2): 257–259. doi:10.1111/jdv.12187. PMID 23682576.
- Stryer, Lubert (1995). In: Biochemistry (Fourth ed.). New York: W.H. Freeman and Company. p. 707. ISBN 0-7167-2009-4.
- Le, T.; Bhushan, V.; Sochat, M.; Kallianos, K.; Chavda, Y.; Zureick, A. H.; Kalani, M. (2017). First aid for the USMLE step 1 2017. New York: Mcgraw-Hill Education. ISBN 978-1259837630.
- "Parathyroid Adenoma". Archived from the original on 2011-07-16.
- Carrol, Mary F.; David S. Schade (1 May 2003). "A Practical Approach to Hypercalcemia". American Family Physician. 67 (9): 1959–1966. PMID 12751658. Archived from the original on 21 August 2014.
his constellation of symptoms has led to the mnemonic “Stones, bones, abdominal moans, and psychic groans,” which is used to recall the signs and symptoms of hypercalcemia, particularly as a result of primary hyperparathyroidism.
- McConnell, Thomas H. (2007). The Nature of Disease: Pathology for the Health Professions. Lippincott Williams & Wilkins. p. 466. ISBN 9780781753173.
"Stones" refers to kidney stones, "bones" to associated destructive bone changes, "groans" to the pain of stomach and peptic ulcers that occur in some cases, and "moans" to the depression that frequently accompanies the disease and is often its first and most prominent manifestation.
- Marx SJ. (2011) Hyperparathyroid Genes: Sequences Reveal Answers and Questions. Endocr. Pract.
- Sulaiman L, Nilsson IL, Juhlin CC, Haglund F, Höög A, Larsson C, Hashemi J (June 2012). "Genetic characterization of large parathyroid adenomas". Endocr Relat Cancer. 19 (3): 389–407. doi:10.1530/ERC-11-0140. PMC 3359501. PMID 22454399.
- Pomerantz JM (2010). "Hyperparathyroidism Resulting From Lithium Treatment Remains Underrecognized". Drug Benefit Trends. 22: 62–63. Archived from the original on 2010-07-01.
- Zink AR, Panzer S, Fesq-Martin M, Burger-Heinrich E, Wahl J, Nerlich AG (2001). "Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications". Endocr. Rev. 22 (4): 477–501. doi:10.1210/er.22.4.477. PMID 11493580.
- Bilezikian JP, Silverberg SJ. Clinical practice. Asymptomatic primary hyperparathyroidism. N Engl J Med. 2004 Apr 22;350(17):1746-51
- "Archived copy" (PDF). Archived (PDF) from the original on 2014-10-05. Retrieved 2014-10-29.CS1 maint: archived copy as title (link)
- Ott, SM (April 1998). "Calcimimetics–new drugs with the potential to control hyperparathyroidism". J. Clin. Endocrinol. Metab. 83 (4): 1080–2. doi:10.1210/jc.83.4.1080. PMID 9543121.
- Ballinger, AE; Palmer, SC; Nistor, I; Craig, JC; Strippoli, GF (9 December 2014). "Calcimimetics for secondary hyperparathyroidism in chronic kidney disease patients". The Cochrane Database of Systematic Reviews. 12 (12): CD006254. doi:10.1002/14651858.CD006254.pub2. PMID 25490118.
- Zink AR, Panzer S, Fesq-Martin M, Burger-Heinrich E, Wahl J, Nerlich AG (2005). "Evidence for a 7000-year-old case of primary hyperparathyroidism". JAMA. 293 (1): 40–2. doi:10.1001/jama.293.1.40-c. PMID 15632333.
External links
| Classification | |
|---|---|
| External resources |
- Hyperparathyroidism at Curlie
- Overview at Endocrine and Metabolic Diseases Information Service
- Insogna KL (September 2018). "Primary Hyperparathyroidism". N. Engl. J. Med. (Review). 379 (11): 1050–59. CiteSeerX 10.1.1.322.5883. doi:10.1056/NEJMcp1714213. PMID 30207907.