Skin condition
A skin condition, also known as cutaneous condition, is any medical condition that affects the integumentary system—the organ system that encloses the body and includes skin, hair, nails, and related muscle and glands.[1] The major function of this system is as a barrier against the external environment.[2]
| Skin condition | |
|---|---|
| Other names | Cutaneous condition |
| Specialty | Dermatology |
Conditions of the human integumentary system constitute a broad spectrum of diseases, also known as dermatoses, as well as many nonpathologic states (like, in certain circumstances, melanonychia and racquet nails).[3][4] While only a small number of skin diseases account for most visits to the physician, thousands of skin conditions have been described.[5] Classification of these conditions often presents many nosological challenges, since underlying causes and pathogenetics are often not known.[6][7] Therefore, most current textbooks present a classification based on location (for example, conditions of the mucous membrane), morphology (chronic blistering conditions), cause (skin conditions resulting from physical factors), and so on.[8][9]
Clinically, the diagnosis of any particular skin condition is made by gathering pertinent information regarding the presenting skin lesion(s), including the location (such as arms, head, legs), symptoms (pruritus, pain), duration (acute or chronic), arrangement (solitary, generalized, annular, linear), morphology (macules, papules, vesicles), and color (red, blue, brown, black, white, yellow).[10] The diagnosis of many conditions often also requires a skin biopsy which yields histologic information[11][12] that can be correlated with the clinical presentation and any laboratory data.[13][14] The introduction of cutaneous ultrasound has allowed the detection of cutaneous tumors, inflammatory processes, nail disorders and hair diseases.[15]
Layer of skin involved
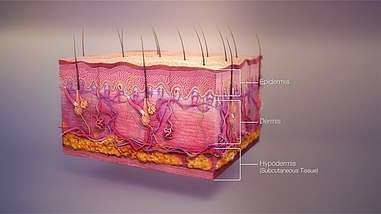
The skin weighs an average of 4 kg (8.8 lb), covers an area of 2 m2 (22 sq ft), and is made of three distinct layers: the epidermis, dermis, and subcutaneous tissue.[1] The two main types of human skin are glabrous skin, the nonhairy skin on the palms and soles (also referred to as the "palmoplantar" surfaces), and hair-bearing skin.[16] Within the latter type, hairs in structures called pilosebaceous units have a hair follicle, sebaceous gland, and associated arrector pili muscle.[17] In the embryo, the epidermis, hair, and glands are from the ectoderm, which is chemically influenced by the underlying mesoderm that forms the dermis and subcutaneous tissues.[18][19][20]
Epidermis
The epidermis is the most superficial layer of skin, a squamous epithelium with several strata: the stratum corneum, stratum lucidum, stratum granulosum, stratum spinosum, and stratum basale.[21] Nourishment is provided to these layers via diffusion from the dermis, since the epidermis is without direct blood supply.[22] The epidermis contains four cell types: keratinocytes, melanocytes, Langerhans cells, and Merkel cells. Of these, keratinocytes are the major component, constituting roughly 95% of the epidermis.[16] This stratified squamous epithelium is maintained by cell division within the stratum basale, in which differentiating cells slowly displace outwards through the stratum spinosum to the stratum corneum, where cells are continually shed from the surface.[16] In normal skin, the rate of production equals the rate of loss; about two weeks are needed for a cell to migrate from the basal cell layer to the top of the granular cell layer, and an additional two weeks to cross the stratum corneum.[23]
Dermis
The dermis is the layer of skin between the epidermis and subcutaneous tissue, and comprises two sections, the papillary dermis and the reticular dermis.[24] The superficial papillary dermis interdigitates with the overlying rete ridges of the epidermis, between which the two layers interact through the basement membrane zone.[24] Structural components of the dermis are collagen, elastic fibers, and ground substance also called extra fibrillar matrix.[24] Within these components are the pilosebaceous units, arrector pili muscles, and the eccrine and apocrine glands.[21] The dermis contains two vascular networks that run parallel to the skin surface—one superficial and one deep plexus—which are connected by vertical communicating vessels.[21][25] The function of blood vessels within the dermis is fourfold: to supply nutrition, to regulate temperature, to modulate inflammation, and to participate in wound healing.[26][27]
Subcutaneous tissue
The subcutaneous tissue is a layer of fat between the dermis and underlying fascia.[5] This tissue may be further divided into two components, the actual fatty layer, or panniculus adiposus, and a deeper vestigial layer of muscle, the panniculus carnosus.[16] The main cellular component of this tissue is the adipocyte, or fat cell.[5] The structure of this tissue is composed of septal (i.e. linear strands) and lobular compartments, which differ in microscopic appearance.[21] Functionally, the subcutaneous fat insulates the body, absorbs trauma, and serves as a reserve energy source.[5]
Diseases of the skin
Diseases of the skin include skin infections and skin neoplasms (including skin cancer).[28]
History
In 1572, Geronimo Mercuriali of Forlì, Italy, completed De morbis cutaneis (translated "On the diseases of the skin"). It is considered the first scientific work dedicated to dermatology.
Diagnoses
The physical examination of the skin and its appendages, as well as the mucous membranes, forms the cornerstone of an accurate diagnosis of cutaneous conditions.[29] Most of these conditions present with cutaneous surface changes termed "lesions," which have more or less distinct characteristics.[30] Often proper examination will lead the physician to obtain appropriate historical information and/or laboratory tests that are able to confirm the diagnosis.[29] Upon examination, the important clinical observations are the (1) morphology, (2) configuration, and (3) distribution of the lesion(s).[29] With regard to morphology, the initial lesion that characterizes a condition is known as the "primary lesion," and identification of such a lesions is the most important aspect of the cutaneous examination.[30] Over time, these primary lesions may continue to develop or be modified by regression or trauma, producing "secondary lesions."[1] However, with that being stated, the lack of standardization of basic dermatologic terminology has been one of the principal barriers to successful communication among physicians in describing cutaneous findings.[21] Nevertheless, there are some commonly accepted terms used to describe the macroscopic morphology, configuration, and distribution of skin lesions, which are listed below.[30]
Lesions
Primary lesions

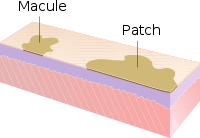

- Macule: A macule is a change in surface color, without elevation or depression and, therefore, nonpalpable, well or ill-defined,[31] variously sized, but generally considered less than either 5[31] or 10 mm in diameter at the widest point.[30]
- Patch: A patch is a large macule equal to or greater than either 5 or 10 mm across,[30] depending on one's definition of a macule.[1] Patches may have some subtle surface change, such as a fine scale or wrinkling, but although the consistency of the surface is changed, the lesion itself is not palpable.[29]
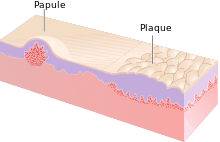
- Papule: A papule is a circumscribed, solid elevation of skin with no visible fluid, varying in size from a pinhead to less than either 5[31] or 10 mm in diameter at the widest point.[30]
- Plaque: A plaque has been described as a broad papule, or confluence of papules equal to or greater than 10 mm,[30] or alternatively as an elevated, plateau-like lesion that is greater in its diameter than in its depth.[29]
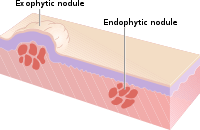
- Nodule: A nodule is morphologically similar to a papule in that it is also a palpable spherical lesion less than 10 mm in diameter. However, it is differentiated by being centered deeper in the dermis or subcutis.
- Tumour: Similar to a nodule but larger than 10 mm in diameter.
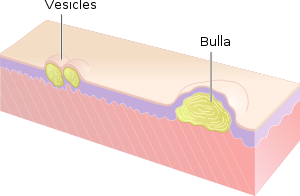
- Vesicle: A vesicle is small blister,[32] a circumscribed, fluid-containing, epidermal elevation generally considered less than either 5[31] or 10 mm in diameter at the widest point.[30] The fluid is clear serous fluid.
- Bulla: A bulla is a large blister,[32] a rounded or irregularly shaped blister containing serous or seropurulent fluid, equal to or greater than either 5[31] or 10 mm,[30] depending on one's definition of a vesicle.[1]
- Pustule: A pustule is a small elevation of the skin containing cloudy[29] or purulent material (pus) usually consisting of necrotic inflammatory cells.[30] These can be either white or red.
- Cyst: A cyst is an epithelial-lined cavity containing liquid, semi-solid, or solid material.[31]
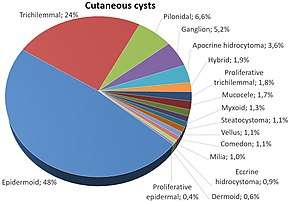 Relative incidence of skin cysts
Relative incidence of skin cysts
- Wheal: A wheal is a rounded or flat-topped, pale red papule or plaque that is characteristically evanescent, disappearing within 24 to 48 hours. The temporary raised bubble of taut skin on the site of a properly-delivered intradermal injection is also called a welt, with the ID injection process itself frequently referred to as simply "raising a wheal" in medical texts.[31]
- Telangiectasia: A telangiectasia represents an enlargement of superficial blood vessels to the point of being visible.[29]
- Burrow: A burrow appears as a slightly elevated, grayish, tortuous line in the skin, and is caused by burrowing organisms.[29][30]
Secondary lesions
- Scale: dry or greasy laminated masses of keratin[30] that represent thickened stratum corneum.[29]
- Crust: dried sebum, pus, or blood usually mixed with epithelial and sometimes bacterial debris.[31]
- Lichenification: epidermal thickening characterized by visible and palpable thickening of the skin with accentuated skin markings.[1]
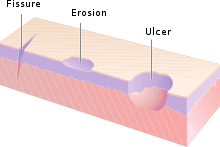
- Erosion: An erosion is a discontinuity of the skin exhibiting incomplete loss of the epidermis,[33] a lesion that is moist, circumscribed, and usually depressed.[21][34]
- Excoriation: a punctate or linear abrasion produced by mechanical means (often scratching), usually involving only the epidermis, but commonly reaching the papillary dermis.[30][34]
- Ulcer: An ulcer is a discontinuity of the skin exhibiting complete loss of the epidermis and often portions of the dermis and even subcutaneous fat.[33][34]
- Fissure: A fissure is a crack in the skin that is usually narrow but deep.[29][34]
- Induration: dermal thickening causing the cutaneous surface to feel thicker and firmer.[29]
- Atrophy: refers to a loss of tissue, and can be epidermal, dermal, or subcutaneous.[30] With epidermal atrophy, the skin appears thin, translucent, and wrinkled.[29] Dermal or subcutaneous atrophy is represented by depression of the skin.[29]
- Maceration: softening and turning white of the skin due to being consistently wet.
- Umbilication: formation of a depression at the top of a papule, vesicle, or pustule.[35]
- Phyma: A tubercle on any external part of the body, such as in phymatous rosacea
Configuration
"Configuration" refers to how lesions are locally grouped ("organized"), which contrasts with how they are distributed (see next section).
- Agminate: in clusters
- Annular or circinate: ring-shaped
- Arciform or arcuate: arc-shaped
- Digitate: with finger-like projections
- Discoid or nummular: round or disc-shaped
- Figurate: with a particular shape
- Guttate: resembling drops
- Gyrate: coiled or spiral-shaped
- Herpetiform: resembling herpes
- Linear
- Mammillated: with rounded, breast-like projections
- Reticular or reticulated: resembling a net
- Serpiginous: with a wavy border
- Stellate: star-shaped
- Targetoid: resembling a bullseye
- Verrucous: wart-like
Distribution
"Distribution" refers to how lesions are localized. They may be confined to a single area (a patch) or may exist in several places. Some distributions correlate with the means by which a given area becomes affected. For example, contact dermatitis correlates with locations where allergen has elicited an allergic immune response. Varicella zoster virus is known to recur (after its initial presentation as chicken pox) as herpes zoster ("shingles"). Chicken pox appears nearly everywhere on the body, but herpes zoster tends to follow one or two dermatomes; for example, the eruptions may appear along the bra line, on either or both sides of the patient.
- Generalized
- Symmetric: one side mirrors the other
- Flexural: on the front of the fingers
- Extensor: on the back of the fingers
- Intertriginous: in an area where two skin areas may touch or rub together
- Morbilliform: resembling measles
- Palmoplantar: on the palm of the hand or bottom of the foot
- Periorificial: around an orifice such as the mouth
- Periungual/subungual: around or under a fingernail or toenail
- Blaschkoid: following the path of Blaschko's lines in the skin
- Photodistributed: in places where sunlight reaches
- Zosteriform or dermatomal: associated with a particular nerve
Other related terms
- Collarette
- Comedo
- Confluent
- Eczema (a type of dermatitis)
- Evanescent (lasting less than 24 hours)
- Granuloma
- Livedo
- Purpura
- Erythema (redness)
- Horn (a cell type)
- Poikiloderma
Histopathology
References
- Miller, Jeffrey H.; Marks, James G. (2006). Lookingbill and Marks' Principles of Dermatology. Saunders. ISBN 1-4160-3185-5.
- Lippens, S; Hoste, E; Vandenabeele, P; Agostinis, P; Declercq, W (April 2009). "Cell death in the skin". Apoptosis. 14 (4): 549–69. doi:10.1007/s10495-009-0324-z. PMID 19221876.
- King, L.S. (1954). "What Is Disease?". Philosophy of Science. 21 (3): 193–203. doi:10.1086/287343.
- Bluefarb, Samuel M. (1984). Dermatology. Upjohn Co. ISBN 0-89501-004-6.
- Lynch, Peter J. (1994). Dermatology. Williams & Wilkins. ISBN 0-683-05252-7.
- Tilles G, Wallach D (1989). "[The history of nosology in dermatology]". Ann Dermatol Venereol (in French). 116 (1): 9–26. PMID 2653160.
- Lambert WC, Everett MA (October 1981). "The nosology of parapsoriasis". J. Am. Acad. Dermatol. 5 (4): 373–95. doi:10.1016/S0190-9622(81)70100-2. PMID 7026622.
- Jackson R (1977). "Historical outline of attempts to classify skin diseases". Can Med Assoc J. 116 (10): 1165–68. PMC 1879511. PMID 324589.
- Copeman PW (February 1995). "The creation of global dermatology". J R Soc Med. 88 (2): 78–84. PMC 1295100. PMID 7769599.
- Fitzpatrick, Thomas B.; Klauss Wolff; Wolff, Klaus Dieter; Johnson, Richard R.; Suurmond, Dick; Richard Suurmond (2005). Fitzpatrick's color atlas and synopsis of clinical dermatology. McGraw-Hill Medical Pub. Division. ISBN 0-07-144019-4.
- Werner B (August 2009). "[Skin biopsy and its histopathologic analysis: Why? What for? How? Part I]". An Bras Dermatol (in Portuguese). 84 (4): 391–95. doi:10.1590/s0365-05962009000400010. PMID 19851671.
- Werner B (October 2009). "[Skin biopsy with histopathologic analysis: why? what for? how? part II]". An Bras Dermatol (in Portuguese). 84 (5): 507–13. doi:10.1590/S0365-05962009000500010. PMID 20098854.
- Xiaowei Xu; Elder, David A.; Rosalie Elenitsas; Johnson, Bernett L.; Murphy, George E. (2008). Lever's Histopathology of the Skin. Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 978-0-7817-7363-8.
- Weedon's Skin Pathology, 2-Volume Set: Expert Consult – Online and Print. Edinburgh: Churchill Livingstone. 2009. ISBN 978-0-7020-3941-6.
- Fernando Alfageme, Cerezo E, Roustan G. "Real-Time Elastography in Inflammatory Skin Diseases: A Primer Ultrasound" in Medicine & Biology, Volume 41, Issue 4, Supplement, April 2015, pp. S82–S83
- Burns, Tony; et al. (2006) Rook's Textbook of Dermatology CD-ROM. Wiley-Blackwell. ISBN 1-4051-3130-6.
- Paus R, Cotsarelis G (1999). "The biology of hair follicles". N Engl J Med. 341 (7): 491–97. doi:10.1056/NEJM199908123410706. PMID 10441606.
- Goldsmith, Lowell A. (1983). Biochemistry and physiology of the skin. Oxford University Press. ISBN 0-19-261253-0.
- Fuchs E (February 2007). "Scratching the surface of skin development". Nature. 445 (7130): 834–42. Bibcode:2007Natur.445..834F. doi:10.1038/nature05659. PMC 2405926. PMID 17314969.
- Fuchs E, Horsley V (April 2008). "More than one way to skin ". Genes Dev. 22 (8): 976–85. doi:10.1101/gad.1645908. PMC 2732395. PMID 18413712.
- Wolff, Klaus Dieter; et al. (2008). Fitzpatrick's Dermatology in General Medicine. McGraw-Hill Medical. ISBN 978-0-07-146690-5.
- "Skin Anatomy". Medscape. Retrieved 3 June 2013.
- Bolognia, Jean L.; et al. (2007). Dermatology. St. Louis: Mosby. ISBN 978-1-4160-2999-1.
- Rapini, Ronald P. (2005). Practical dermatopathology. Elsevier Mosby. ISBN 0-323-01198-5.
- Grant-Kels, JM (2007). Color Atlas of Dermatopathology (Dermatology: Clinical & Basic Science). Informa Healthcare. p. 163. ISBN 978-0-8493-3794-9.
- Ryan, T (1991). "Cutaneous Circulation". In Goldsmith, Lowell A (ed.). Physiology, biochemistry, and molecular biology of the skin (2nd ed.). New York: Oxford University Press. p. 1019. ISBN 0-19-505612-4.
- Swerlick, RA; Lawley, TJ (January 1993). "Role of microvascular endothelial cells in inflammation". J. Invest. Dermatol. 100 (1): 111S–115S. doi:10.1038/jid.1993.33. PMID 8423379.
- Rose, Lewis C. (1998-09-15). "ecognizing Neoplastic Skin Lesions: A Photo Guide". American Family Physician. 58 (4): 873–84, 887–8. PMID 9767724. Retrieved 3 June 2013.
- Callen, Jeffrey (2000). Color atlas of dermatology. Philadelphia: W.B. Saunders. ISBN 0-7216-8256-1.
- James, William D.; et al. (2006). Andrews' Diseases of the Skin: Clinical Dermatology. Saunders Elsevier. ISBN 0-7216-2921-0.
- Fitzpatrick, Thomas B.; Klauss Wolff; Wolff, Klaus Dieter; Johnson, Richard R.; Suurmond, Dick; Richard Suurmond (2005). Fitzpatrick's color atlas and synopsis of clinical dermatology. New York: McGraw-Hill Medical Pub. Division. ISBN 0-07-144019-4.
- Elsevier, Dorland's Illustrated Medical Dictionary, Elsevier.
- Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease. St. Louis, Mo: Elsevier Saunders. ISBN 0-7216-0187-1.
- Copstead, Lee-Ellen C.; Diestelmeier, Ruth E.; Diestelmeier, Michael R. (2016-09-03). "Alterations in the Integumentary System". Basicmedical Key. Retrieved 2019-07-01.
- "Description of Skin Lesions". The Merk Manual. Retrieved 3 June 2013.