Mortality rate
Mortality rate, or death rate,[3]:189,69 is a measure of the number of deaths (in general, or due to a specific cause) in a particular population, scaled to the size of that population, per unit of time. Mortality rate is typically expressed in units of deaths per 1,000 individuals per year; thus, a mortality rate of 9.5 (out of 1,000) in a population of 1,000 would mean 9.5 deaths per year in that entire population, or 0.95% out of the total. It is distinct from "morbidity", which is either the prevalence or incidence of a disease, and also from the incidence rate (the number of newly appearing cases of the disease per unit of time).[3]:189
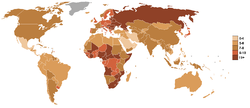
An important specific mortality rate measure is the crude death rate, which looks at mortality from all causes in a given time interval for a given population. As of 2020, for instance, the CIA estimates that the crude death rate globally will be 7.7 deaths per 1,000 persons in a population per year.[4] In a generic form,[3]:189 mortality rates can be seen as calculated using , where d represents the deaths from whatever cause of interest is specified that occur within a given time period, p represents the size of the population in which the deaths occur (however this population is defined or limited), and is the conversion factor from the resulting fraction to another unit (e.g., multiplying by to get mortality rate per 1,000 individuals).[3]:189



Crude death rate, globally
The crude death rate is defined as "the mortality rate from all causes of death for a population," calculated as the "[t]otal number of deaths during a given time interval" divided by the "[m]id-interval population", per 1,000 or 100,000; for instance, the population of the U.S. was ca. 290,810,000 in 2003, and in that year, approximately 2,419,900 deaths occurred in total, giving a crude death (mortality) rate of 832 deaths per 100,000.[5]:3–20f As of 2020, the CIA estimates the U.S. crude death rate will be 8.3 per 1,000, while it estimates that the global rate will be 7.7 per 1,000.[4]
According to the World Health Organization, the ten leading causes of death, globally, in 2016, for both sexes and all ages, were as presented in the table below.[6]
Crude death rate, per 100,000 population
- Ischaemic heart disease, 126
- Stroke, 77
- Chronic obstructive pulmonary disease, 41
- Lower respiratory infections, 40
- Alzheimer's disease and other dementias, 27
- Trachea, bronchus, lung cancers, 23
- Diabetes mellitus, 21
- Road injury, 19
- Diarrhoeal diseases, 19
- Tuberculosis, 17
Related measures of mortality
Other specific measures of mortality include:[5]
| Name | Typical definition |
|---|---|
| Perinatal mortality rate | The sum of fetal deaths (stillbirths) past 22 (or 28) completed weeks of pregnancy plus the number of deaths among live-born children up to 7 completed days of life, divided by number of births.[7] |
| Maternal mortality rate | Number of deaths assigned to pregnancy-related causes during a given time interval, divided by the number of live births during the same time interval.[5]:3–20 |
| Infant mortality rate | Number of deaths among children < 1 year of age during a given time interval divided by the number of live births during the same time interval.[5]:3–20 |
| Child mortality rate (also known as 'Under-five mortality rate') | Number of deaths of children less than 5 years old, divided by number of live births.[8] |
| Standardized mortality ratio (SMR) | The ratio of the number of deaths in a given (index) population to the number of deaths expected, a form of indirectly (as opposed to directly) standardized rates, where the categories are usually "defined by age, gender and race or ethnicity".[9] The numerator is calculated as , where " is the number of persons in category of the index population and is the corresponding category-specific event rate in a standard population."[9][9] It has also been described as a proportional comparison to the numbers of deaths that would have been expected if the population had been of a standard composition in terms of age, gender, etc.[10] |
| Age-specific mortality rate (ASMR) | The total number of deaths per year at a specific age, divided by the number of living persons at that age (e.g. age 62 at last birthday)[5]:3–21 |
| Cause-specific death rate | Number of deaths assigned to a specific cause during a given time interval divided by the mid-interval population[5]:3–21 |
| Cumulative death rate | The incidence proportion of death, that is, the proportion of a [defined] group that dies over a specified time interval,[3]:64 whether in reference to all deaths over the time inverval, to "to deaths from a specific cause or causes".[3]:64 It has also been described as a measure of the (growing) proportion of a group that die over a specified period (often as estimated by techniques that account for missing data by statistical censoring). |
| Case fatality rate (CFR) | The proportion of diagnosed cases of a particular medical condition that lead to death.[11] |
| Infection fatality rate (IFR) | The proportion of infected cases of a particular medical condition that lead to death. Similar to CFR, but adjusted for asymptomatic and undiagnosed cases.[12] |




For any of these, a "sex-specific mortality rate" refers to "a mortality rate among either males or females", where the calculation involves both "numerator and denominator... limited to the one sex".[5]:3–23
Use in epidemiology
In most cases there are few if any ways to obtain exact mortality rates, so epidemiologists use estimation to predict correct mortality rates. Mortality rates are usually difficult to predict due to language barriers, health infrastructure related issues, conflict, and other reasons. Maternal mortality has additional challenges, especially as they pertain to stillbirths, abortions, and multiple births. In some countries, during the 1920s, a stillbirth was defined as "a birth of at least twenty weeks' gestation in which the child shows no evidence of life after complete birth". In most countries, however, a stillbirth was defined as "the birth of a fetus, after 28 weeks of pregnancy, in which pulmonary respiration does not occur".[13]
Census data and vital statistics
Ideally, all mortality estimation would be done using vital statistics and census data. Census data will give detailed information about the population at risk of death. The vital statistics provide information about live births and deaths in the population.[14] Often, either census data and vital statistics data is not available. This is especially true in developing countries, countries that are in conflict, areas where natural disasters have caused mass displacement, and other areas where there is a humanitarian crisis [14]
Household surveys
Household surveys or interviews are another way in which mortality rates are often assessed. There are several methods to estimate mortality in different segments of the population. One such example is the sisterhood method, which involves researchers estimating maternal mortality by contacting women in populations of interest and asking whether or not they have a sister, if the sister is of child-bearing age (usually 15) and conducting an interview or written questions about possible deaths among sisters. The sisterhood method, however, does not work in cases where sisters may have died before the sister being interviewed was born.[15]
Orphanhood surveys estimate mortality by questioning children are asked about the mortality of their parents. It has often been criticized as an adult mortality rate that is very biased for several reasons. The adoption effect is one such instance in which orphans often do not realize that they are adopted. Additionally, interviewers may not realize that an adoptive or foster parent is not the child's biological parent. There is also the issue of parents being reported on by multiple children while some adults have no children, thus are not counted in mortality estimates.[14]
Widowhood surveys estimate adult mortality by responding to questions about the deceased husband or wife. One limitation of the widowhood survey surrounds the issues of divorce, where people may be more likely to report that they are widowed in places where there is the great social stigma around being a divorcee. Another limitation is that multiple marriages introduce biased estimates, so individuals are often asked about first marriage. Biases will be significant if the association of death between spouses, such as those in countries with large AIDS epidemics.[14]
Sampling
Sampling refers to the selection of a subset of the population of interest to efficiently gain information about the entire population. Samples should be representative of the population of interest. Cluster sampling is an approach to non-probability sampling; this is an approach in which each member of the population is assigned to a group (cluster), and then clusters are randomly selected, and all members of selected clusters are included in the sample. Often combined with stratification techniques (in which case it is called multistage sampling), cluster sampling is the approach most often used by epidemiologists. In areas of forced migration, there is more significant sampling error. Thus cluster sampling is not the ideal choice.[16]
Mortality statistics
Causes of death vary greatly between developed and less developed countries; see also list of causes of death by rate for worldwide statistics.
| Years | CDR | Years | CDR |
|---|---|---|---|
| 1950–1955 | 19.1 | 2000–2005 | 8.4 |
| 1955–1960 | 17.3 | 2005–2010 | 8.1 |
| 1960–1965 | 16.2 | 2010–2015 | 8.1 |
| 1965–1970 | 12.9 | 2015–2020 | 8.1 |
| 1970–1975 | 11.6 | 2020–2025 | 8.1 |
| 1975–1980 | 10.6 | 2025–2030 | 8.3 |
| 1980–1985 | 10.0 | 2030–2035 | 8.6 |
| 1985–1990 | 9.4 | 2035–2040 | 9.0 |
| 1990–1995 | 9.1 | 2040–2045 | 9.4 |
| 1995–2000 | 8.8 | 2045–2050 | 9.7 |
The ten countries with the highest crude death rate, according to the 2016 CIA World Factbook estimates, are:[18]
| Rank | Country | Death rate (annual deaths/1,000 persons) |
|---|---|---|
| 1 | 14.9 | |
| 2 | 14.5 | |
| 3 | 14.5 | |
| 4 | 14.4 | |
| 5 | 14.4 | |
| 6 | 14.1 | |
| 7 | 14.0 | |
| 8 | 13.7 | |
| 9 | 13.6 | |
| 10 | 13.6 |
According to Jean Ziegler (the United Nations Special Rapporteur on the Right to Food for 2000 to March 2008), mortality due to malnutrition accounted for 58% of the total mortality in 2006: "In the world, approximately 62 million people, all causes of death combined, die each year. In 2006, more than 36 million died of hunger or diseases due to deficiencies in micronutrients".[19]
Of the roughly 150,000 people who die each day across the globe,[20][21][22] about two thirds—100,000 per day—die of age-related causes.[23] In industrialized nations, the proportion is much higher, reaching 90%.[23]
Economics
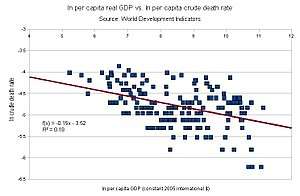
Scholars have stated that there is a significant relationship between a low standard of living that results from low income; and increased mortality rates. A low standard of living is more likely to result in malnutrition, which can make people more susceptible to disease and more likely to die from these diseases. A lower standard of living may lead to as a lack of hygiene and sanitation, increased exposure to and the spread of disease, and a lack of access to proper medical care and facilities. Poor health can in turn contribute to low and reduced incomes, which can create a loop known as the health-poverty trap.[24] Indian economist and philosopher Amartya Sen has stated that mortality rates can serve as an indicator of economic success and failure.[25][26]:27, 32
Historically, mortality rates have been adversely affected by short term price increases. Studies have shown that mortality rates increase at a rate concurrent with increases in food prices. These effects have a greater impact on vulnerable, lower-income populations than they do on populations with a higher standard of living.[26]:35–36, 70
In more recent times, higher mortality rates have been less tied to socio-economic levels within a given society, but have differed more between low and high-income countries. It is now found that national income, which is directly tied to standard of living within a country, is the largest factor in mortality rates being higher in low-income countries.[27]
These rates are especially pronounced for children under 5 years old, particularly in lower-income, developing countries. These children have a much greater chance of dying of diseases that have become very preventable in higher-income parts of the world. More children die of malaria, respiratory infections, diarrhea, perinatal conditions, and measles in developing nations. Data shows that after the age of 5 these preventable causes level out between high and low-income countries.
See also
- Biodemography
- Compensation law of mortality
- Demography
- Gompertz–Makeham law of mortality
- List of causes of death by rate
- List of countries by birth rate
- List of countries by death rate
- List of countries by life expectancy
- Maximum life span
- Micromort
- Mortality displacement
- Risk adjusted mortality rate
- Vital statistics
- Medical statistics
- Weekend effect
- World population
References
- "Archived copy". Archived from the original on 2013-06-03. Retrieved 2020-01-31.CS1 maint: archived copy as title (link)
- "World Population Prospects, the 2010 Revision". September 26, 2011. Archived from the original on 2011-09-26.
- Porta, M, ed. (2014). "Mortality Rate, Morbidity rate; Death rate; Cumulative death rate; Case fatality rate". A Dictionary of Epidemiology (5th ed.). Oxford: Oxford University Press. pp. 189, 69, 64, 36. ISBN 978-0-19-939005-2.
- CIA Staff (2020). "People and Society". CIA World Factbook. Retrieved January 31, 2020.
- For tabulated definitions for Crude death rate, Cause-specific death rate, Proportionate mortality, Death-to-case ratio, Neonatal mortality rate, Postneonatal mortality rate, Infant mortality rate, and Maternal mortality rate (with example calculations for several), see Dicker, Richard C.; Coronado, Fátima; Koo, Denise; Parrish II, Roy Gibson (2012). "Lesson Three: Measures of Risk, §Mortality Frequency Measures" (PDF). Principles of Epidemiology in Public Health Practice: An Introduction to Applied Epidemiology and Biostatistics. Atlanta, GA: U.S. Department of HHS, Centers for Disease Control and Prevention (CDC). pp. 3–20 to 3–38. Retrieved January 31, 2020.CS1 maint: uses authors parameter (link)
- WHO Staff (2018). "Global Health Observatory (GHO) data: Top 10 causes of death". Geneva, CH: World Health Organization. Retrieved January 31, 2020.
- "Perinatal Mortality". 2008. Retrieved 2020-03-30.
- "Global Health Observatory (GHO) data – Under-five mortality". Retrieved 2020-03-30.
- Gail, Mitchell & Benichou, Jacques (2000). "Standardized mortality ratio (SMR)" (PDF). Encyclopedia of Epidemiologic Methods. Wiley Reference Series in Biostatistics. New York, NY: John Wiley & Sons. p. 884. ISBN 9780471866411. Retrieved January 31, 2020.CS1 maint: uses authors parameter (link)
- Everitt, B.S. The Cambridge Dictionary of Statistics. Cambridge, UK: Cambridge University Press. ISBN 052181099X.
- "Principles of Epidemiology - Lesson 3: Measures of Risk Section 3: Mortality Frequency Measures". Centers for disease control and prevention. U.S. Department of Health & Human Services. 18 February 2019. Retrieved 25 March 2020.
- "Infection fatality rate". DocCheck Medical Services GmbH. Retrieved 25 March 2020.
- Loudon, Irvine (1992). Death in Childbirth: An International Study of Maternal Care and Maternal Mortality 1800–1950 – Oxford Scholarship. Oxford University Press. doi:10.1093/acprof:oso/9780198229971.001.0001. ISBN 9780191678950.
- Timæus, Ian M. (1991). "Measurement of Adult Mortality in Less Developed Countries: A Comparative Review". Population Index. 57 (4): 552–568. doi:10.2307/3644262. JSTOR 3644262.
- Graham, W.; Brass, W.; Snow, R. W. (May 1989). "Estimating maternal mortality: the sisterhood method". Studies in Family Planning. 20 (3): 125–135. doi:10.2307/1966567. ISSN 0039-3665. JSTOR 1966567. PMID 2734809.
- Migration, National Research Council (US) Roundtable on the Demography of Forced (2002). Estimating Mortality Rates. National Academies Press (US).
- "UNdata - record view - Crude death rate (deaths per 1,000 population)". data.un.org.
- "The World Factbook — Central Intelligence Agency – Country Comparison: Death Rate". www.cia.gov.
- Jean Ziegler, L'Empire de la honte, Fayard, 2007 ISBN 978-2-253-12115-2, p.130.
- "Civil registration: why counting births and deaths is important". www.who.int. Retrieved 2020-06-11.
- "Global deaths: This is how COVID-19 compares to other diseases". World Economic Forum. Retrieved 2020-06-11.
- Ross, Jenna (2020-05-15). "How Many People Die Each Day?". Visual Capitalist. Retrieved 2020-06-11.
- Aubrey D.N.J, de Grey (2007). "Life Span Extension Research and Public Debate: Societal Considerations" (PDF). Studies in Ethics, Law, and Technology. 1 (1, Article 5). CiteSeerX 10.1.1.395.745. doi:10.2202/1941-6008.1011. Archived from the original (PDF) on October 13, 2016. Retrieved August 7, 2011.
- "Health, Income, & Poverty: Where We Are & What Could Help". October 4, 2018. doi:10.1377/hpb20180817.901935. Cite journal requires
|journal=(help) - Sen, Amartya (1998). "Mortality as an Indicator of Economic Success and Failure". The Economic Journal. 108 (446): 1–25. doi:10.1111/1468-0297.00270. ISSN 0013-0133. JSTOR 2565734.
- Bengtsson, Tommy; Campbell, Cameron; Lee, James Z. (2004). Life under pressure: mortality and living standards in Europe and Asia, 1700–1900. Cambridge, MA: MIT. ISBN 978-0262268097. OCLC 57141654.
- Preston, Samuel H. (2007-06-01). "The changing relation between mortality and level of economic development". International Journal of Epidemiology. 36 (3): 484–490. doi:10.1093/ije/dym075. ISSN 0300-5771. PMC 2572360. PMID 17550952.
Sources
- Crude death rate (per 1,000 population) based on World Population Prospects The 2008 Revision, United Nations. Retrieved 22 June 2010
- Rank Order – Death rate in CIA World Factbook
- Mortality in The Medical Dictionary, Medterms. Retrieved 22 June 2010
- "WISQARS Leading Causes of Death Reports, 1999–2007", US Centers for Disease Control Retrieved 22 June 2010
- Edmond Halley, An Estimate of the Degrees of the Mortality of Mankind (1693)
External links
| Wikimedia Commons has media related to Mortality rates. |
- DeathRiskRankings: Calculates risk of dying in the next year using MicroMorts and displays risk rankings for up to 66 causes of death
- Data regarding death rates by age and cause in the United States (from Data360)
- Complex Emergency Database (CE-DAT): Mortality data from conflict-affected populations
- Human Mortality Database: Historic mortality data from developed nations
| In medicine |
| ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lists | |||||||||||||
| Mortality | |||||||||||||
| After death |
| ||||||||||||
| Paranormal | |||||||||||||
| Legal | |||||||||||||
| Fields | |||||||||||||
| Other |
| ||||||||||||
| |||||||||||||