Cyclothymia
Cyclothymia, also known as cyclothymic disorder, is a mental disorder that involves numerous periods of symptoms of depression and periods of symptoms of hypomania.[3] These symptoms, however, are not sufficient to be a major depressive episode or a hypomanic episode.[3] Symptoms must last for more than one year in children and two years in adults.[3]
| Cyclothymia | |
|---|---|
| Other names | Cyclothymic disorder |
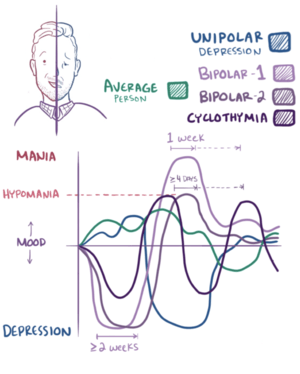 | |
| Graphical representation of cyclothymia compared with bipolar disorder and major depression | |
| Specialty | Psychiatry, clinical psychology |
| Symptoms | Periods of depression and elevated mood[1] |
| Complications | Suicide, self-harm[1] |
| Causes | Unknown[2] |
| Risk factors | Family history[3] |
| Differential diagnosis | Bipolar disorder, borderline personality disorder, substance misuse disorder[3] |
| Treatment | Psychotherapy, medications[4] |
| Frequency | 0.4-1% at some point in life[3] |
The cause of cyclothymia is unknown.[2] Risk factors include a family history of bipolar disorder.[3] Cyclothymia differs from bipolar in that major depression, mania, or hypomania have never occurred.[3]
Treatment is generally with counselling and mood stabilizers such as lithium.[4] It is estimated that 0.4-1% of people have cyclothymia at some point in their life.[3] Onset is typically in late childhood to early adulthood.[3] Males and females are affected equally often.[3]
Symptoms
People with cyclothymia experience both depressive phases and hypomanic phases (which are less severe than a full hypomanic episode).[3] The depressive and manic symptoms in cyclothymia last for variable amounts of time due to the unstable and reactive nature of the disorder.[1] The depressive phases are similar to major depressive disorder and are characterized by dulled thoughts and sensations and the lack of motivation for intellectual or social activities.[1] Most people with cyclothymia are generally fatigued and tend to sleep frequently and for long periods of time.[1] However, other people experience insomnia.[1]
Other symptoms of cyclothymic depression include indifference toward people or activities that used to be extremely important.[1] Cyclothymic depression also leads to difficulty making decisions.[1] In addition, people with this condition tend to be critical and complain easily.[1] Suicidal thoughts are common, even in mild forms of cyclothymia.[1] In the depressive state, people with cyclothymia also experience physical complaints including frequent headaches, tightness in the head and chest, an empty sensation in the head, weakness, weight loss, and hair loss.[1]
The distinguishing factor between typical depression and cyclothymic depression is that in cyclothymic depression, there are instances of hypomania. People with cyclothymia can switch from the depressive state to the hypomanic state without warning to them or others. The duration and frequency of phases is unpredictable.[1]
In the hypomanic state, people's thoughts become faster and they become more sociable and talkative. They may engage in spending sprees, spontaneous actions, have heightened self-esteem, and greater vanity.[1] In contrast to a regular manic state that would be associated with bipolar I, symptoms in the hypomanic phase generally occur in a less severe form.[1]
Comorbidities
Cyclothymia commonly occurs in conjunction with other disorders.[5] Between 20-50 percent of people with depression, anxiety, and related disorders also have cyclothymia.[4] When people with cyclothymia seek mental health resources it tends to be for symptoms of their comorbid condition rather than for their symptoms of cyclothymia. In children and adolescents, the most common comorbidities with cyclothymia are anxiety disorders, impulse control issues, eating disorders, and ADHD.[4] In adults, cyclothymia also tends to be comorbid with impulse control issues. Sensation-seeking behaviors occur in hypomanic states.[5] These often include gambling and compulsive sexuality in men, or compulsive buying and binge eating in women.[5]
In addition to sensation-related disorders, cyclothymia has also been associated with atypical depression. In one study, a connection was found between interpersonal sensitivity, mood reactivity (i.e., responding to actual or potential positive events with brighter mood), and cyclothymic mood swings,[5] all of which are symptoms of atypical depression. Cyclothymia also tends to occur in conjunction with separation anxiety, where a person has anxiety as a result of separation from a caregiver, friend, or loved one. Other issues that tend to co-occur with cyclothymia include social anxiety, fear of rejection and a tendency toward hostility to those connected with past pain and rejection. People with cyclothymia tend to seek intense interpersonal relationships when in a hypomanic state and isolation when in a depressed state.[5] This generally leads to short, tumultuous relationships.[5]
Causes
The cause is unknown.[2] Risk factors include a family history of bipolar disorder.[3]
First-degree relatives of people with cyclothymia have major depressive disorder, bipolar I disorder, and bipolar II disorder more often than the general population. Substance-related disorders also may be at a higher risk within the family. First-degree relatives of a bipolar I individuals may have a higher risk of cyclothymic disorder than the general population.[6]
Diagnosis
Cyclothymia is classified in DSM-5 as a subtype of bipolar disorder. The criteria are:[7]
- Periods of elevated mood and depressive symptoms for at least half the time during the last two years for adults and one year for children and teenagers.
- Periods of stable moods last only two months at most.
- Symptoms create significant problems in one or more areas of life.
- Symptoms do not meet the criteria for bipolar disorder, major depression, or another mental disorder.
- Symptoms are not caused by substance use or a medical condition.
The DSM-5 criteria for cyclothymia are restrictive according to some researchers.[5] This affects the diagnosis of cyclothymia because fewer people get diagnosed than potentially could.[5] This means that a person who has some symptoms of the disorder might not be able to get treatment because they do not meet all of the necessary criteria described in DSM-5.[5] Furthermore, it also leads to more attention being placed on depression and other bipolar-spectrum disorders because if a person does not meet all the criteria for cyclothymia they are often given a depression or bipolar spectrum diagnosis.[5] Improper diagnosis may lead some people with cyclothymia to be treated for a comorbid disorder rather than having their cyclothymic tendencies addressed.[5]
Cyclothymia is often not recognized by the affected individual or medical professionals due to its ostensibly mild symptoms. In addition, it is difficult to identify and classify. Due to disagreement and misconceptions among health and mental health professionals, cyclothymia is often diagnosed as "bipolar not otherwise specified". Cyclothymia is also often confused with borderline personality disorder due to their similar symptoms,[8] especially in older adolescents and young adults.
Most people with the disorder present in a depressive state, not realizing that their hypomanic states are abnormal.[1] Mild manic episodes tend to be interpreted as part of the person's personality or simply a heightened mood. In addition, the disorder often manifests during childhood or adolescence, making it even more difficult for the person to distinguish between symptoms of the disorder and their personality. For example, people may think that they just suffer from mood swings and not realize that these are a result of a psychiatric condition.[5]
Management
Cognitive behavioral therapy (CBT) is considered potentially effective for people diagnosed with cyclothymia.[4]
Medication can be used in addition to behavioral approaches. However, mood stabilizers should be used before antidepressants, and if antidepressants are used they should be used with caution.[4] Antidepressants are a concern due to the possibility of inducing hypomanic switches or rapid cycling.[4]
History
In 1883, Karl Ludwig Kahlbaum identified a disorder characterized by recurring mood cycles. The disorder contained both melancholic and manic episodes that occurred in a milder form than in bipolar disorder.[9] This condition was coined "cyclothymia" by Kahlbaum and his student Ewald Hecker.[1] Kahlbaum developed his theory of cyclothymia through his work with people presenting with these symptoms at the Kahlbaum Sanitarium in Goerlitz, Silesia (Germany).[1] He was recognized as a leading hypnotherapist and psychotherapist of his day.[1] He was a progressive in the field of mental health, believing that mental illness should not carry a stigma and that people dealing with mental health issues should be treated humanely.[1] Kalhbaum was the first to recognize that people with cyclothymia often do not seek help for the disorder due to its mild symptoms.[1]
Cyclothymia has been conceptualized in a variety of ways, including as a subtype of bipolar disorder, a temperament, a personality trait, and a personality disorder.[10] There is also an argument that cyclothymia should be considered a neurodevelopmental disorder.[4] The two defining features of the disorder, according to DSM-5, are the presence of depressive episodes and hypomania. Cyclothymia is also classified as a subtype of bipolar disorder in DSM-5, but some researchers disagree with this classification and argue that it should be primarily defined as an exaggeration of mood and emotional instability.[5] In the past, cyclothymia has been conceptualized to include other characteristics in addition to the flux between depression and hypomania, such as mood reactivity, impulsivity, and anxiety.[5]
Epidemiology
Cyclothymia, known today as cyclothymic disorder, tends to be underdiagnosed due to its low intensity.[5] The exact rates for cyclothymia have not been widely studied.[5] Some studies estimate that between 5 and 8% are affected at some point in their life whereas other studies suggest a rate ranging from 0.4 to 2.5%.[5]
Males appear to be affected equally often,[3] though women are more likely to receive treatment.[5] Cyclothymia is diagnosed in around fifty percent of people with depression who are evaluated in psychiatric outpatient settings.[5]
Etymology
Cyclothymia is derived from the Greek word κυκλοθυμία (from κῦκλος kyklos, "circle"[11] and θυμός thymos, "mood, emotion").[12] Therefore, it means "to cycle or circle between moods or emotions".
Research
Whether subtypes of bipolar disorder, such as cyclothymia, truly represent separate disorders or are part of a unique bipolar spectrum is debated in research. Cyclothymia is typically not described in research studies or diagnosed in clinical settings, making it less recognizable and less understood by professionals. This absence of cyclothymia in research and clinical settings suggests that cyclothymia is either being diagnosed as another mood disorder or as a non-affective psychiatric disorder or not coming to scientific or clinical attention[13] due to a lack of diagnostic clarity or because the nature of cyclothymia is still highly contested. Additionally, the current diagnostic criterion for cyclothymia emphasizes that symptoms are persistent, which suggests that they are enduring traits rather than a psychological state, thus, it has been argued that it should be diagnosed as a personality disorder. Since the symptoms tend to overlap with personality disorders, the validity and distinction between these two diagnostic categories has been debated.[14]
Lastly, the tendency of cyclothymia to be comorbid with other mental disorders makes diagnosis difficult.[13] These issues prevent consensus on the definition of cyclothymia and its relationship with other mental disorders among researchers and clinicians. This lack of consensus on an operational definition and symptom presentation is especially pronounced with children and adolescents because the diagnostic criteria have not been adequately adapted to take into account their developmental level.[15]
Society and culture
Actor Stephen Fry has spoken about his experience with cyclothymia, which was depicted in the documentary Stephen Fry: The Secret Life of the Manic Depressive.[16]
Singer Charlene Soraia had cyclothymia and wrote a song about her experiences with the disorder.[17]
See also
References
- Koukopoulos, A (January 2003). "Ewald Hecker's description of cyclothymia as a cyclical mood disorder: its relevance to the modern concept of bipolar II". Journal of Affective Disorders. 73 (1–2): 199–205. doi:10.1016/S0165-0327(02)00326-9. PMID 12507752.
- "Cyclothymia". nhs.uk. 2017-10-18. Retrieved 20 May 2018.
- American Psychiatric Association (2013), Diagnostic and Statistical Manual of Mental Disorders (5th ed.), Arlington: American Psychiatric Publishing, pp. 139–141, ISBN 978-0890425558
- Perugi, G; Hantouche, E; Vannucchi, G (April 2017). "Diagnosis and Treatment of Cyclothymia: The "Primacy" of Temperament". Current Neuropharmacology. 15 (3): 372–379. doi:10.2174/1570159X14666160616120157. PMC 5405616. PMID 28503108.
- Perugi, G; Hantouche, E; Vannucchi, G; Pinto, O (1 September 2015). "Cyclothymia reloaded: A reappraisal of the most misconceived affective disorder". Journal of Affective Disorders. 183: 119–33. doi:10.1016/j.jad.2015.05.004. PMID 26005206.
- DSM-5 (2013), Risk and Prognostic Factors, p. 141
- Diagnostic and statistical manual of mental disorders : DSM-5 (5th ed.). Washington, D.C.: American Psychiatric Association. 2013. ISBN 978-0-89042-554-1.
- Kaplan & Sadock’s Comprehensive Textbook of Psychiatry (2017), 13.1 Mood Disorders: Historical Introduction and Conceptual Overview => Dysthymia and Cyclothymia. "It is not always easy to demarcate full-blown syndromal episodes of depression and mania from their subthreshold counterparts commonly observed during the interepisodic periods. The subthreshold conditions appear to be fertile terrain for interpersonal conflicts and postaffective pathological character developments that may ravage the lives of patients and their families. In North America and some Western European countries many such patients end up being labeled with borderline personality disorder, which, unfortunately, often tends to obscure the affective origin of the presenting psychopathology."
- Commentary on Hecker and his work: Baethge, C; Salvatore, P; Baldessarini, RJ (September 2003). "Cyclothymia, a circular mood disorder". History of Psychiatry. 14 (55 Pt 3): 377–390. doi:10.1177/0957154X030143008. PMID 14621693. New translation of Hecker's 1898 paper: Hecker, Ewald; Salvatore, P; Baldessarini, R. J. (September 2003). "Classic Text No 55: Cyclothymia, a Circular Mood Disorder by Hecker, 1898". History of Psychiatry. 14 (55 Pt 3): 391–399. doi:10.1177/0957154X030143008. PMID 14621693.
- Parker, G; McCraw, S; Fletcher, K (June 2012). "Cyclothymia". Depression and Anxiety. 29 (6): 487–94. doi:10.1002/da.21950. PMID 22553122.
- κύκλος, Henry George Liddell, Robert Scott, A Greek-English Lexicon, on Perseus
- θυμός, Henry George Liddell, Robert Scott, A Greek-English Lexicon, on Perseus
- Danner, Stephanie; Mary A. Fristad; L. Eugene Arnold; Eric A. Youngstrom; Boris Birmaher; Sarah M. Horwitz; Christine Demeter; Robert L. Findling; Robert A. Kowatch (2009). "Early-Onset Bipolar Spectrum Disorders: Diagnostic Issues". Clinical Child and Family Psychology Review. 12 (3): 271–93. doi:10.1007/s10567-009-0055-2. PMC 3575107. PMID 19466543.
- Sass, H.; Juneman, K. (2003). "Affective disorders, personality and personality disorders". Acta Psychiatr Scand. 108 (418): 34–40. doi:10.1034/j.1600-0447.108.s418.8.x. PMID 12956812.
- Avenevoli, Shelli (2009). "Bipolar Disorder in Children and Adolescents: New Data to Inform Classification". NIMH. Archived from the original on 27 April 2018. Retrieved 26 April 2018.
- "Stephen Fry: The Secret Life of the Manic Depressive (but I have cyclothymia)". BBC - Health. Archived from the original on 2010-01-12. Retrieved 2018-12-21.
- Copsey, Robert. "Ones to watch: Charlene Soraia". London: Digital Spy. Retrieved 21 December 2018.
Cited sources
- Sadock, Benjamin; Sadock, Virginia; Ruiz, Pedro, eds. (2017). "13. Mood Disorders". Kaplan and Sadock's Comprehensive Textbook of Psychiatry (10th ed.). New York: Wolters Kluwer.