Oroantral fistula
Oroantral fistula (OAF) is an epithelialised oroantral communication (OAC).[1] OAC refers to an abnormal connection between the oral cavity and antrum (or maxillary sinus).[1] The creation of an OAC is most commonly due to the extraction of a maxillary (upper) tooth (typically a maxillary first molar) closely related to the antral floor (floor of the maxillary sinus).[1] A small OAC (up to 5mm wide) may heal spontaneously but a larger OAC would require surgical closure to prevent the development of persistent OAF and chronic sinusitis.[1]
| Oroantral fistula | |
|---|---|
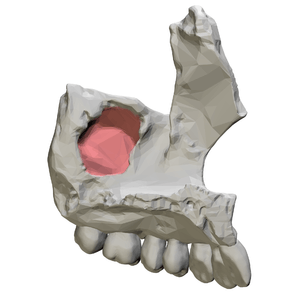 | |
| Maxillary sinus (medial view) | |
| Specialty | ENT surgery |
Classification
| OAC | OAF |
|---|---|
| Connection between oral cavity and antrum that is not epithelialised. | Connection between oral cavity and antrum that has epithelialised. |
| May develop immediately following the extraction of maxillary tooth that is close to antral floor. | Develops from OAC that has not healed spontaneously, has not been closed surgically, or initial attempts at surgical closure have failed. |
| Requires surgical closure if large to prevent development of a persistent OAF and chronic sinusitis. | Requires surgical treatment to remove and close the fistula. |
Signs and symptoms of an OAC/OAF can include the following
When looking in the mouth, a communication in the upper jaw (i.e. a hole) can be seen connecting the mouth to the maxillary sinus.[2] Sometimes this can be the only sign, as pain (+/- other symptoms) is not always present.
Symptoms
· Same side nose blockage (unilateral nasal obstruction).[2] When an OAC or OAF is present, the passage to the maxillary sinus can results in infection and inflammation in the maxillary sinus. This subsequently results in mucus build up presenting as a unilateral nasal blockage
· Sinusitis can progress – this can present as a pain in the midface. Pain can be referred to the upper teeth and be mistaken for toothache[3]
· Fluid can flow from the mouth through the communication and into the maxillary sinus. The maxillary sinus is connected to the nose and therefore fluid can come out of the nostrils when drinking[2]
· Change in sounds produced from the nose and the voice – specifically a whistling sound whilst speaking[2]
· Taste can be affected[2]
Signs
· Visible hole between mouth and sinus
· Fracture of the floor of the maxillary sinus creating a communication to the oral cavity (e.g. as seen following trauma).[2]
· Air bubbles, blood or mucoid secretion around the orifice can be seen as air passes from the sinus into the oral cavity through the communication.
Diagnosis
- Patient history - Diagnosis is usually based on clinical examination and reported symptoms. Therefore, a good history and understanding of the patient’s symptoms is key.
- Undertake a complete extraoral and intraoral examination using a dental mirror alongside good lightening. When assessing the socket following an extraction look for granulation tissue in the socket which may represent normal healing. Assess for the presence of visible an opening/hole between the oral cavity and the maxillary sinus.
- Imaging can be useful. However, radiographs only show if there is a breach in the bony floor of the antrum. Even if there is a breach in the bony floor then the Schneiderian membrane may still be intact. Depending on the size of the potential communication and in what context, a small radiograph inside the mouth may be sufficient (a periapical) to assess for any break in the bone of the sinus floor which may indicate an OAC.
- Panoramic radiographs[2] can also be used to confirm the presence of an OAC. If simple radiographs are deemed not to give enough information, cone beam computed tomography (CBCT)[2] (special x-ray equipment that can scan in 3 dimensions) may be used. Imaging can help locate the communication, determine the size of it and can give an indication as to whether there is any sinusitis and foreign bodies in the sinus.
- Normally clinicians should be cautioned against probing or irrigating the site a newly formed OAC as this may reduce the chance of spontaneous healing.
- Valsalva test (nose blowing test)[4] The patient is asked to pinch their nostrils together and open their mouth and then blow gently through the nose. The clinician must observe if there is passage of air or bubbling of blood in the post extraction alveolus as the trapped air from closed nostrils is forced into the mouth through any oroantral communication. Gentle suction applied to the socket often produces a characteristic hollow sound. However, there are differing opinions about the appropriateness of carrying out this test. It can be argued that by performing this test, a small OAC may be made bigger thus preventing spontaneous healing.
Causes
Extraction of maxillary teeth
The maxillary sinus is known for its thin floor and close proximity to the posterior maxillary (upper) teeth.[1][5] The extraction of a maxillary tooth (typically a maxillary first molar which lies close to the lowest point of antral floor although any premolar or molar can be affected) is the most common cause of an OAC (which can then progress to an OAF as described above).[1] Extraction of primary teeth are not considered a risk of OAC due to the presence of developing permanent teeth and the small size of the developing maxillary sinus.[1]
Other causes
Other causes of an OAC are: maxillary fractures across the antral floor typically Le Fort I, displacement of posterior maxillary molar roots into antrum and direct trauma.[5] An OAC can happen for many other more unusual reasons, such as acute or chronic inflammatory lesions around the tip of a tooth root which is in close proximity with the maxillary antrum, destructive lesions/tumours of the maxilla, failure of surgical incisions to heal (e.g. Caldwell-luc antrostomy), osteomyelitis of the maxilla, careless use of instruments during surgical procedures, Syphilis, implants and as a results of complex surgery (for example removal of a large cysts or resections of large tumours involving the maxilla.[6][7][8]
Diagnosis
Clinical examination and x rays can help diagnose the condition. For examples :
- Valsalva test (nose blowing test):[9] Ask the patient to pinch the nostrils together and open the mouth, then blow gently through the nose. Observe if there is passage of air or bubbling of blood in the post extraction alveolus as the trapped air from closed nostrils is forced into the mouth through any oroantral communication. Gentle suction applied to the socket often produces a characteristic hollow sound.
- Perform a complete extra- and intra-oral examination using a dental mirror under good lighting, look for granulation tissue in the socket and openings into the antrum.
- Panoramic radiograph or paranasal computed tomography can help to locate the fistula, the size of it and to determine the presence of sinusitis and other foreign bodies. Other methods like radiographs (occipitomental, OPG and periapical views) can also be used to confirm the presence of any oroantral fistulas.
- To test the patency of communication the patient is asked to rinse the mouth or water is flushed in the tooth socket.
- Unilateral epistaxis is seen in case of collection of blood in the sinus cavity.
- Do not probe or irrigate the site, because it may lead to sinusitis or push foreign bodies, such as contaminated fragments, or oral flora further into the antrum. Hence, leading to the formation of a new fistula or widen an existing one.
Complications
OAF is a complication of oroantral communication. Other complications may arise if left untreated. For example:
- Candidal infection[9][10]
- Chronic maxillary sinus infection of bacterial origin[11]
- Osteomyelitis[12]
- Rhinosinusitis[13]
- Sinus pathology[9]
Therefore, OAF should be dealt with first, before treating the complications.
Prevention
Whilst in some circumstances, preventing development of an OAF following extraction of a tooth can be difficult, careful assessment is important. The following should be considered prior to carrying out any dental treatment:[1]
- Size of the antrum and proximity to teeth – this can be assessed radiographically
- Shape and size of teeth and roots – this can be assessed radiographically
- Presence of periapical pathology – this can be assessed radiographically
- The age of the patient
- The patient’s past dental history
If the above factors are assessed as increasing the risk of OAC development, the clinician should take appropriate steps to carefully remove the tooth in question, possibly carrying out a surgical extraction and in an appropriate setting.[1] Hence, in such cases:
- Avoid using too much of apical pressure during tooth extraction
- Perform surgical extraction with roots sectioning
- Consider referral to OMFS at local hospital[1]
Treatment
The primary aim of treatment of a newly formed oroantral communication is to prevent the development of an oroantral fistula as well as chronic sinusitis. The decision on how to treat OAC/OAF depends on various factors. Small size communications between 1 and 2 mm in diameter, if uninfected, are likely to form a clot and heal by itself later. Communications larger than this require treatments to close the defect and these interventions can be categorised into 3 types: surgical, non-surgical and pharmacological.[14][15]
Surgery
Surgical methods are required if a large defect is present or if a defect persists.[16] Surgery involves creating a flap utilising local tissue to close the communication. There are a number of different flaps that can be used such as the buccal advancement flap, the buccal fat pad flap, a combination of the two and a palatal flap.[16] The flap used is dependent on the size and position of the defect.
Buccal advancement flap
The buccal advancement flap is the most commonly used due to its simplicity, reliability and versatility.[16] It involves cutting a broad based trapezoid shaped mucoperiosteal flap with two vertical incisions.[16] The flap is cut buccally, is three sided and extends to the full depth of the sulcus.[1]
Buccal fat pad flap
The buccal fat pad flap is also a popular option due to its high success rate.[17] It is a simple procedure where the buccal extension of the anatomical fat pad is used for closure.[2] These two flaps can be used in combination where the buccal fat pad covers the communication followed by a further covering via the buccal mucosal flap described above.[2] This double layer flap has advantages over a single layer as it provides stable soft tissue covering, reduces the incidences of wound breakdown and defect recurrence as well as reducing the risk of postoperative infection.[2]
Sutures, either non-resorbing or slowly resorbing, are generally used in the surgical repairs of OAC.[1]
Non-surgical interventions
Ultimately, surgery is usually required to close an OAC/OAF. However, if surgery is not immediately available then non-surgical methods can be used to encourage the growth of oral mucosa between the oral cavity and the antrum.[1] The aim of these methods is to protect the blood clot within the socket and help to prevent infection. One option is construction of a denture with an acrylic base plate or extension of the patient’s existing denture to protect the socket and support the clot.[1] These options are particularly helpful in patients who smoke as it provides protection from smoke inhalation. The socket can also be sutured over with mattress sutures if there is adequate soft tissue available.[1]
Medication
Medications may be needed as an adjunct to assist the closure of the defect. Antibiotics can help control or prevent any sinus infections. Preoperative nasal decongestants usage can reduce any existing sinus inflammation which will aid surgical manipulation of the mucosa over the bone.[18]
Postoperative care
Following all methods of OAC/OAF closure, the patients are instructed to avoid activities that could produce pressure changes between the nasal passages and oral cavity for at least 2 weeks due to risk of disruption to the healing process. Nose blowing and sneezing with a closed mouth are prohibited. A soft diet is also often advocated during this period. Following surgery, nasal decongestants and prophylactic antibiotics are often prescribed to prevent postoperative infection.
References
- Pedlar J, Frame JW (2007). Oral and maxillofacial surgery: an objective-based textbook (2nd ed.). Edinburgh: Elsevier/Churchill Livingstone. ISBN 978-0-443-10073-4. OCLC 698080410.
- Khandelwal P, Hajira N (January 2017). "Management of Oro-antral Communication and Fistula: Various Surgical Options". World Journal of Plastic Surgery. 6 (1): 3–8. PMC 5339603. PMID 28289607.
- Renton T (January 2020). "Tooth-Related Pain or Not?". Headache. 60 (1): 235–246. doi:10.1111/head.13689. PMID 31675112.
- Sandhya G, Reddy PB, Kumar KA, Sridhar Reddy B, Prasad N, Kiran G (September 2013). "Surgical Management of Oro-Antral Communications Using Resorbable GTR Membrane and FDMB Sandwich Technique: A Clinical Study". Journal of Maxillofacial and Oral Surgery. 12 (3): 254–9. doi:10.1007/s12663-012-0437-8. PMC 3777032. PMID 24431851.
- Coulthard P, Horner K, Sloan P, Theaker ED (2013-05-17). Oral and maxillofacial surgery, radiology, pathology and oral medicine. Master Dentistry. 1 (Third ed.). Edinburgh. ISBN 978-0-7020-4600-1. OCLC 826658944.
- Balaji SM (2007). Textbook of oral and maxillofacial surgery. New Delhi [India]: Elsevier. ISBN 978-81-312-0300-2. OCLC 779906048.
- Malik NA (2008). Textbook of oral and maxillofacial surgery (2nd ed.). New Delhi: Jaypee. ISBN 978-81-8448-157-0. OCLC 868917979.
- DeFreitas J, Lucente FE (December 1988). "The Caldwell-Luc procedure: institutional review of 670 cases: 1975-1985". The Laryngoscope. 98 (12): 1297–300. doi:10.1288/00005537-198812000-00004. PMID 3200074.
- Jadhav KB, Mujib BA, Gupta N (January 2014). "Cytological approach for diagnosis of non-healing oroantral fistula associated with candidiasis". Journal of Cytology. 31 (1): 47–9. doi:10.4103/0970-9371.130704. PMC 4150343. PMID 25190985.
- Nilesh K, Malik NA, Belgaumi U (April 2015). "Mucormycosis in a healthy elderly patient presenting as oro-antral fistula: Report of a rare incidence". Journal of Clinical and Experimental Dentistry. 7 (2): e333-5. doi:10.4317/jced.52064. PMC 4483347. PMID 26155356.
- Bell G (August 2011). "Oro-antral fistulae and fractured tuberosities". British Dental Journal. 211 (3): 119–23. doi:10.1038/sj.bdj.2011.620. PMID 21836575.
- Gannepalli A, Ayinampudi BK, Baghirath PV, Reddy GV (2015-09-15). "Actinomycotic Osteomyelitis of Maxilla Presenting as Oroantral Fistula: A Rare Case Report". Case Reports in Dentistry. 2015: 689240. doi:10.1155/2015/689240. PMC 4586902. PMID 26451261.
- Mishra AK, Sinha VR, Nilakantan A, Singh DK (June 2016). "Rhinosinusitis associated with post-dental extraction chronic oroantral fistula: outcomes of non-surgical management comprising antibiotics and local decongestion therapy". The Journal of Laryngology and Otology. 130 (6): 545–53. doi:10.1017/S0022215116001213. PMID 27150223.
- Dym H, Wolf JC (May 2012). "Oroantral communication". Oral and Maxillofacial Surgery Clinics of North America. 24 (2): 239–47, viii–ix. doi:10.1016/j.coms.2012.01.015. PMID 22503070.
- Vinod K (2004-01-01). Textbook of oral and maxillofacial surgery. Arya (Medi) Pub. House. ISBN 9788186809082. OCLC 703144522.
- Parvini P, Obreja K, Sader R, Becker J, Schwarz F, Salti L (December 2018). "Surgical options in oroantral fistula management: a narrative review". International Journal of Implant Dentistry. 4 (1): 40. doi:10.1186/s40729-018-0152-4. PMC 6306369. PMID 30588578.
- Batra H, Jindal G, Kaur S (March 2010). "Evaluation of different treatment modalities for closure of oro-antral communications and formulation of a rational approach". Journal of Maxillofacial and Oral Surgery. 9 (1): 13–8. doi:10.1007/s12663-010-0006-y. PMC 3453686. PMID 23139559.
- von Wowern N (June 1982). "Closure of oroantral fistula with buccal flap: Rehrmann versus Môczár". International Journal of Oral Surgery. 11 (3): 156–65. doi:10.1016/s0300-9785(82)80003-3. PMID 6813275.
External links
| Classification |
|---|