Pre-exposure prophylaxis
Pre-exposure prophylaxis (PrEP) is a term used to describe the use of medications used to prevent the spread of disease in people who have not yet been exposed to a disease-causing agent, usually a virus. The term typically refers to the specific use of antiviral drugs as a strategy for HIV/AIDS prevention.[1]

PrEP is one of a number of HIV prevention strategies for people who are HIV negative but who also have higher risk of acquiring HIV, including sexually active adults at increased risk of HIV, people who engage in injection drug use (see drug injection), and serodiscordant sexually active couples.[2] Other strategies can include the use of condoms, as well as harm reduction methods of using clean resources provided by safe injection sites and needle exchange programs.[3]
As of 2019, the World Health Organization (WHO) recommends two drug combinations for the use as PrEP for HIV/AIDS: the combination of tenofovir disoproxil and emtricitabine (Truvada), or the combination of tenofovir disoproxil and lamivudine (Cimduo).[4] In October 2019, the U.S. Food and Drug Administration (FDA) approved the combination of emtricitabine and tenofovir alafenamide (Descovy) to be used as PrEP in addition to Truvada, which provides similar levels of protection.[5]
When used as directed, PrEP has been shown to be highly effective, reducing the risk of acquiring HIV up to 99%.[6]
Medical uses
In the United States, federal guidelines recommend the use of pre-exposure prophylaxis (PrEP) for HIV-negative adults with the following characteristics:
- sexually active in the last 6 months and NOT in a sexually monogamous relationship with a recently tested HIV-negative partner, and who...[2]
- is a man who has sex with men, and who...
- has had anal sex with another man in the past 6 months without a condom, or...
- has had a sexually transmitted infection in the past 6 months
- or is a sexually active adult (male or female with male or female partners), and who...
- is a man who has sex with both men and women, or...
- has sex with partners at increased risk of having HIV (e.g. injection drug users, men who have sex with men) without consistent condom use
- is a man who has sex with men, and who...
- or anyone who has injected illicit drugs in the past six months, shared recreational drug injection equipment with other drug users in the past six months, or who has been in treatment for injection drug use in the past six months
Other government health agencies from around the world have devised their own national guidelines for how to use PrEP to prevent HIV infection in those at high risk, including Botswana, Canada, Kenya, Lesotho, South Africa, Uganda, the United Kingdom, Zambia, and Zimbabwe.[7]
Often, lab testing is required before starting PrEP, including a test for HIV. Once PrEP is initiated, individuals are asked to see their provider at least every three to six months. During those visits, healthcare providers may want to repeat testing for HIV, test for other sexually transmitted infections, monitor kidney function, and/or test for pregnancy.[2] Individuals must test negative for HIV prior to PrEP initiation, because persons infected with HIV taking PrEP medication are at risk for becoming resistant to emtricitabine. Consequently, these people with HIV infection and resistance to emtricitabine will have less options for selecting HIV treatment medications.[8]
PrEP has been shown to be effective at reducing the risk of acquiring HIV in individuals at increased risk.[2] However, PrEP is not 100% effective at preventing HIV, even in people who take the medication as prescribed.[9] There have been several reported cases of people who acquired HIV despite taking PrEP.[10] People taking PrEP may use combination prevention strategies along with PrEP, like condoms.[2] If someone on PrEP acquires HIV, they may experience the Signs and symptoms of HIV/AIDS.[11]
PrEP is typically taken continuously and daily following potential exposure. The CDC recommends follow-up visits at least every 3 months to provide HIV tests, medication adherence counseling, behavioral risk reduction support, side effect assessment, STI symptom assessment, and STI testing for sexually active individuals with symptoms of a current infection. Pregnancy tests should also be done every 3 months for woman who may become pregnant. At 3 months and every 6 months thereafter, renal function and presence of bacterial STI is assessed.[12] Effectiveness of PrEP is associated with adherence, with effectiveness decreasing with suboptimal adherence.[13]
Although the daily, oral dosing schedule is still recommended for all individuals taking PrEP medication for HIV infection prevention, event-driven pre-exposure prophylaxis, or ED-PrEP, is an option for men who have sex with men. ED-PrEP is also referred to as "2+1+1" dosing, because the dosing regimen involves a person taking two pills two to twenty-four hours prior to sex, one pill twenty-four hours after taking the first two pills, and a last pill taken forty-eight hours after taking the first two pills.[14] This dosing regimen was first proven effective to reduce the relative risk of HIV infection by 86% in the IPERGAY randomized clinical trial performed in Canada and France in 2015. According to the WHO, ED-PrEP should be considered for HIV infection prevention in men who have sex with men who have relatively infrequent sex, who are able to plan sex or delay sex for about two hours, and who find this dosing schedule convenient. ED-PrEP is not recommended for use in other populations, such as cisgender or transgender women and men who have vaginal and/or anal sex with women, due to the lack of safety and efficacy data available studying ED-PrEP in these populations. ED-PrEP can be beneficial to help reduce pill burden for people and decrease costs, as fewer pills are needed.[15]
In 2016, the World Health Organization (WHO) consolidated guidelines regarding the use of antiretroviral drugs for treatment and prevention of HIV infection support the use of PrEP in pregnant and breastfeeding women who are at continued and substantial risk of HIV infection.[16][17] In clinical PrEP trials, exposure to TDF-containing PrEP during the first trimester of pregnancy was not associated with adverse pregnancy or infant outcomes. The increased risk of mother-to-child HIV transmission outweigh any potential risks of PrEP. The guidelines also note the need for continued monitoring of pregnant and breastfeeding women receiving PrEP.[17] However, global PrEP accessibility for women, including those who are either pregnant or breastfeeding, is limited. Efforts to increase accessibility to women who are at risk for HIV are necessary in reducing rates of global HIV infections.[18]
Contraindications
Truvada and Descovy are contraindicated for use as pre-exposure prophylaxis (PrEP) in individuals who have an unknown or positive HIV status.[19][20] HIV positive or negative status must be determined before someone begins the use of either of these medications as PrEP.[19][20] Additionally, any hypersensitivity or severe allergy to any ingredient, emtricitabine, tenofovir disoproxil, or tenofovir alafenamide is a contraindication for continued use of these medications.[19][20]
Side effects
Research shows that pre-exposure prophylaxis (PrEP) is generally safe and well tolerated for most individuals, although some side effects have been noted to occur. Some people experience a "start-up syndrome" involving nausea, headache, and/or stomach issues, which generally resolve within a few weeks of starting the PrEP medication.[2][21] Research has shown that the use of Truvada as PrEP has been associated with mild to moderate declines in kidney function, mostly associated with older people over 50, those with predisposing conditions such as diabetes, or glomerular filtration rate lower than 90.[22][19][23] These declines were usually of no concern, stabilized after several weeks of being on the drug, and reversed once the drug was discontinued.[24][25] However, these side effects were serious enough for several people on PrEP to file lawsuits against the makers of Truvada as well as the makers of other similar drugs.[26][27][28]
Osteopenia or bone loss has been reported in clinical studies.[29][30] Bone loss was not seen as a major concern for ending the service since bone loss was considered minimal and did not lead to osteoporosis.[30] When comparing bone fractures between active participants and control there was no major difference in bone fractures.[30]
Fat redistribution and accumulation was more commonly seen in individuals receiving antiretroviral therapy, particularly older antiretrovirals, for the treatment of HIV.[31] No significant changes in fat redistribution or change in fat has been noted as of now when used as a pre-exposure prophylaxis. Research and study outcome analysis suggests that emtricitabine/tenofovir does not have a significant effect on fat redistribution or accumulation when used as pre-exposure prophylaxis in HIV negative individuals.[32] As of early 2018 these studies have not assessed in detail subtle changes in fat distribution that may be possible with the drug when used as PrEP, and statistically significant - though transient - weight changes have been attributed to detectable drug concentrations in the body.[33]
Other potential serious side effects of Truvada include acute exacerbations of hepatitis B in individuals with HBV infection, lactic acidosis, and severe hepatomegaly with steatosis.[19]
Descovy research and data from public use has shown similar "start-up" effects; however, some data indicates that Descovy is better for one's kidneys and for those with a diagnosis of osteoporosis.[34]
Boxed warnings
Both Truvada and Descovy carry a Black Box Warning for the combination of emtricitabine/tenofovir, as this combination of drugs can result in the acute worsening of hepatitis B infection when discontinued. This combination of drugs is also known to increase HIV resistance to these medications when used as pre-exposure prophylaxis (PrEP) in individuals who are determined to be HIV positive. It is recommended that individuals continue to periodically get tested to determine their HIV status to ensure proper continuing use of these medications for PrEP.[19][20]
Society and culture
Access and adoption
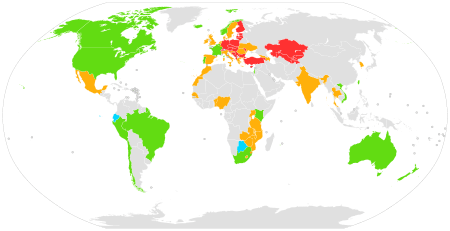
|
Approved
Approved for off-label use
Ongoing and planned demonstration projects
Completed demonstration projects
No planned demonstration project
No data
|
Approval for use
Truvada was previously only approved by the U.S. Food and Drug Administration (FDA) to treat HIV in those already infected. In 2012, the FDA approved the drug for use as pre-exposure prophylaxis (PrEP), based on growing evidence that the drug was safe and effective at preventing HIV in populations at increased risk of infection.[35]
In 2012, the World Health Organization (WHO) issued guidelines for PrEP and made similar recommendations for its use among men and transgender women who have sex with men. The WHO noted that "international scientific consensus is emerging that antiretroviral drugs, including PrEP, significantly reduce the risk of sexual acquisition and transmission of HIV regardless of population or setting."[36]:8,10,11 In 2014, on the basis of further evidence, the WHO updated the recommendation for men who have sex with men to state that PrEP "is recommended as an additional HIV prevention choice within a comprehensive HIV prevention package."[37]:4 In November 2015 the WHO expanded this further, on the basis of further evidence, and stated that it had "broadened the recommendation to include all population groups at substantial risk of HIV infection" and emphasized that PrEP should be "an additional prevention choice in a comprehensive package of services."[38]
As of 2018, numerous countries have approved the use of PrEP for HIV/AIDS prevention, including the United States, South Korea,[39] France, Norway,[40] Australia,[41] Israel,[42] Canada,[42] Kenya, South Africa, Peru, Thailand, the European Union[43][44] and Taiwan.[45]
New Zealand was one of the first countries in the world to publicly fund PrEP for the prevention of HIV in March 2018. Funded access to PrEP will require that people undergo regular testing for HIV and other sexually transmitted infections, and are monitored for risk of side effects. People taking funded PrEP will receive advice on ways to reduce the risk of HIV and sexually transmitted infections.[46]
In Australia, the country's Therapeutic Goods Administration approved the use of Truvada as PrEP in May 2016, allowing Australian providers to legally prescribe the medication. On March 21, 2018, the Federal Minister for Health announced that PrEP will be subsidized by the Australian Government through the Pharmaceutical Benefits Scheme (PBS) from April 1, 2018.[47]
Availability and pricing in the United States
Within the United States, Truvada and Descovy are brand name products of Gilead Sciences that cost around $2200/month (a 30 day supply) at wholesale price.[48][49] In other countries around the world, generic Truvada is available for a much cheaper price. Expected Fall 2020, Teva Pharmaceuticals will begin producing a generic version of Truvada within the United States; however, it has been reported that the details surrounding the rights to the patent are unclear, which makes it difficult to predict if this will increase access to the medications.[50][51] In the meantime, there are several assistance programs at the local, state, and national level for gaining access to PrEP at reduced costs.[52] Gilead has an "advancing access" co-pay coupon program that can be accessed by individuals and providers alike to help cover some of the monthly costs of these medications.[53] It is recommended to discuss other available options with a community pharmacist or physician.
In December 2019, the U.S. announced the Ready, Set, PrEP program to provide free PrEP to the uninsured through major drugstore chains.[54] The Ready, Set, PrEP program is led by the U.S. Department of Health and Human Services (HHS) and allows qualifying individuals to fill their prescription for PrEP medication free of cost at their choice of participating pharmacies or through the mail.[55]
NPIN PrEP Provider Data and Locator Widget was launched on the CDC website to provide a comprehensive, national directory of public and private providers in the U.S. that offer pre-exposure prophylaxis (PrEP) to prevent HIV infection. The database includes over 1,800 PrEP providers from all 50 U.S. states, as well as U.S. territories.[56]
Beginning in January 2020, after California Governor Gavin Newsom signed Senate Bill 159 (SB159) in late 2019, licensed pharmacists in California are authorized to initiate and dispense a 30 to 60 day supply of pre-exposure prophylaxis (PrEP) or the full course of post-exposure prophylaxis (PEP) without a doctor's prescription, given certain clinical criteria of the individual are met. The bill acts as an extension of Medi-Cal benefits (the Medicaid program in the state of California).[57] The law is recognized by pharmacist organizations, health providers, legislators, and the general public to be the removal of a barrier to direct and time-dependent access to these medications, especially for those in communities most affected by HIV/AIDs.[58]
Politics and culture
Since the FDA approval of PrEP for the prevention of HIV, moves toward greater adoption of PrEP have been met some issues, especially around the overall public health effect of widespread adoption, the cost of PrEP and associated disparities in availability and access. Many public health organizations and governments have embraced PrEP as a part of their overall strategy for reducing HIV. For example, in 2014 New York state governor Andrew Cuomo initiated a three-part plan to reduce HIV across New York that specifically emphasized access to PrEP.[59] Similarly, the city of San Francisco launched a "Getting to Zero" campaign. The campaign aims to dramatically reduce the number of new HIV infections in the city and relies on expanding access to PrEP as a key strategy for achieving that goal.[60] Public health officials report that since 2013 the number of new HIV infections in San Francisco has decreased almost 50% and that such improvements are likely related to the city's campaign to reduce new infections.[61] Additionally, numerous public health campaigns have been launched to educate the public about PrEP. For instance, in New York City in 2016 Gay Men's Health Crisis launched an ad campaign in bus shelters across the city reminding riders that adherence to PrEP is important to ensuring the regimen is maximally effective.[62] In Washington, D.C., a PrEP campaign was launched to increase the number of D.C. residents taking PrEP. Social media pushes, such as an ad campaign called "PrEP for Her", targeted African-American women, who, along with gay and bisexual African-American men, are at high risk of infection in the district.[63] Other states and cities that have initiated "Getting to Zero" campaigns include Massachusetts, Connecticut, Illinois, San Diego, Silicon Valley/Santa Clara, and Miami-Dade.[64][65][66][67][68]
Despite those efforts, PrEP remains controversial among some who worry that widespread PrEP adoption could cause public health issues by enabling risky sexual behaviors.[69][70][71] For instance, AIDS Healthcare Foundation founder and director Michael Weinstein has been vocal in his opposition to PrEP adoption, suggesting that PrEP causes people to make riskier decisions about sex than they would otherwise make.[72] Some researchers, however, believe that there is insufficient data to determine whether or not PrEP implementation has an effect on the rate of other sexually transmitted infections.[73] Other critics point out that despite implementation of PrEP, significant disparities exist. For example, some point out that African Americans bear a disproportionate burden of HIV infections but may be less likely than whites to access PrEP.[74] Still other critics of PrEP object to the high cost of the regimen. For example, the U.K.'s NHS initially refused to offer PrEP to individuals citing concerns about cost and suggested that local officials ought to bear the responsibility of paying for the drug. However, following significant advocacy efforts, the NHS has started to offer PrEP to people in the UK in 2017.[75]
Impact on LGBT+ sex culture
PrEP is used predominantly by gay men, often as an alternative to condoms. For the first time since the outbreak of the AIDS crisis, PrEP makes HIV-protected sex without condoms possible and has therefore changed gay sex culture: With the spread of PrEP, condomless sex has increased.[76] But because the condom was for a long time the only effective HIV prevention tool, many gay men do not feel comfortable with condomless sex. Apart from criticisms of PrEP stemming from potential side effects or from concerns that it may raise the risk of spreading sexually transmitted diseases other than HIV, the rejection of PrEP is sometimes connected to a stigma against the acceptability of promiscuous sexuality - a stigma which is present in both online dating platforms such as Grindr, but also to some extent in the media - since PrEP has been perceived to promote promiscuity.[77] PrEP can itself contribute to reducing stigma and (internalized) homophobia, however, because it can help to dissolve the association between gay sex and risk of disease that has been socially prevalent since the outbreak of the AIDS crisis.[78]
Barriers to use
PrEP is globally underutilized. A systematic review of 76 peer-reviewed articles and 28 conference abstracts of values and preferences among global populations who might benefit from PrEP found that awareness of PrEP is low, but individuals were receptive to use when presented with information. Common barriers to PrEP use include lack of communication between an individual and their doctor, stigmatization, concerns about safety, side effects, and cost and effectiveness.[79][80] Transgender women are disproportionally affected by HIV/AIDS,[81] and PrEP is often underutilized. Barriers for PrEP use and access for transgender women include concerns about side effects, cost, hormone therapy, adherence, PrEP-related stigma and interaction with healthcare workers.[82]
Studies evaluating PrEP efficacy to reduce risk of HIV infection found a linear relationship between adherence and effectiveness of medication. This means that the more closely people follow recommended dosing of PrEP, the more effective the medication is at preventing infection. [83]
Research
Most PrEP studies use the drug tenofovir or a tenofovir/emtricitabine combination (Truvada) that is delivered by mouth. Initial studies of PrEP strategies in non-human primates showed a reduced risk of infection among animals that receive ARVs prior to exposure to a simian form of HIV. A 2007 study at UT-Southwestern (Dallas) and the University of Minnesota showed PrEP to be effective in "humanized" laboratory mice.[84] In 2008, the iPrEx study demonstrated 42% reduction of HIV infection among men who have sex with men,[85] and subsequent analysis of the data has suggested that 99% protection is achievable if the drugs are taken every day.[86] Below is a table summarizing some of the major research studies that demonstrated PrEP with Truvada to be effective across different populations.
PrEP approaches with agents besides Truvada are being investigated. There has been some evidence that other regimens, like ones based on the antiretroviral agent Maraviroc, could potentially prevent HIV infection.[87] Similarly, researchers are investigating whether drugs could be used in ways other than a daily pill to prevent HIV, including taking a long-acting PrEP injection, PrEP-releasing implants, or rectally administered PrEP.[88] However, it is important to keep in mind that as of 2017, major public health organizations such as the U.S. Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) recommend only daily Truvada for use as PrEP.[2][38]
Data on efficacy and safety of PrEP in adolescents are insufficient. Risks and benefits of PrEP use should be considered for adolescents.[12]
| Study | Type | Type of PrEP | Study Population | Efficacy | Percent of patients who took medication (adherence) |
|---|---|---|---|---|---|
| CAPRISA 004 | Double-blind, randomized | Pericoital tenofovir gel | South African females | 39% reduction of HIV infection[89] | 72% by applicator count[90] |
| iPrEx | Oral emtricitabine/tenofovir | Men who have sex with men and transgender women | 42% reduction of HIV infection.[85] 99% reduction estimated with daily adherence[86] | 54% detectable in blood[91] | |
| Partners PrEP | Oral emtricitabine/tenofovir; oral tenofovir | African heterosexual couples | Reduction of infection by 73% with Truvada and 62% with tenofovir[92] | 80% with Truvada and 83% with tenofovir[93] detectable in blood | |
| TDF2 | Oral emtricitabine/tenofovir | Botswana heterosexual couples | 63% reduction of infection[21] | 84% by pill count[94] | |
| FEM-PrEP | Oral emtricitabine/tenofovir | African heterosexual females | No reduction (study halted due to low adherence) | <30% with detectable levels in blood[95] | |
| VOICE 003 | Oral emtricitabine/tenofovir; oral tenofovir; vaginal tenofovir gel | African heterosexual females | No reduction in oral tenofovir or vaginal gel arms [oral emtricitabine/tenofovir arm ongoing][21] | <30% with detectable levels in blood[96] | |
| Bangkok Tenofovir Study | Randomized, double-blind | Oral tenofovir | Thai male injection drug users | 48.9% reduction of infection[97] | 84% by directly observed therapy and study diaries[98] |
| IPERGAY | Randomized, double-blind | Oral emtricitabine/tenofovir | French and Quebecois gay males | 86% reduction of infection[99][100] (video summary) | 86% with detectable levels in blood[99] |
| PROUD | Randomized, open-label | Oral tenofovir-emtricitabine | High-risk men who have sex with men in England | 86% reduction of HIV incidence[101] | |
| HPTN 083 | Randomized, double-blind | Cabotegravir versus emtricitabine/tenofovir | Transgender women and cisgender men who have sex with men in Argentina, Brazil, Peru, Thailand, the U.S., Vietnam, and South Africa. | Highly efficacious compared to daily oral TDF/FTC.[102] | |
| Discover study | Randomized, double-blind | oral TDF/FTC versus TAF/FTC | High-risk men who have sex with men in Europe, North and South America | ongoing[103] | |
Possibility of increased risk-taking
While PrEP appears to be extremely successful in reducing HIV infection , there is mixed evidence that there might be a change in use of condoms in anal sex,[104] raising risks of spreading sexually transmitted diseases other than HIV. In a meta-analysis of 18 studies, researchers found that rates of new diagnoses of STIs among MSM (men who have sex with men) given PrEP were 25.3 times greater for gonorrhea, 11.2 times greater for chlamydia and 44.6 times greater for syphilis, compared with the rates among MSM not given PrEP.[105] Unlike HIV, these three STIs can be cured with antibiotics.[106][107][108] However, the increased rates of such infections and their treatment can lead to antibiotic-resistant mutations of the pathogens; antibiotic-resistant gonorrhea is already a major concern.[109]
A systemic review conducted in 2019 was unable to find conclusive evidence that PrEP use increases sexual risk behaviors, and found that PrEP may provide an opportunity for MSM to access sexual health care, testing, treatment and counselling services.[110]
Emerging treatments
Although HIV PrEP medications are only available in oral tablet formulations, other formulations are being developed and studied. The emerging treatments expand HIV prevention strategies for women. For example, a vaginal gel formulation of tenofovir and an intravaginal ring releasing dapivirine are under investigation for efficacy.[14] Out of three completed trials evaluating safety and efficacy of tenofovir vaginal gel, only the CAPRISA 004 trial showed the drug to be efficacious in decreasing the risk of HIV infection. However, the demonstrated effectiveness of tenofovir vaginal gel was deemed not significant enough to move forward with the product. In contrast, the ASPIRE study and The Ring Study evaluating the dapivirine-releasing intravaginal ring have demonstrated efficacy in reducing incidence of HIV infection. In addition to these two treatments, an injectable form of cabotegravir is being evaluated for efficacy in the HPTN 03 and HPTN 04 trials.[111]
References
- "Pre-Exposure Prophylaxis". HIV.gov. 3 December 2019. Retrieved 3 August 2020.
- US Public Health Service. "Preexposure prophylaxis for the prevention of HIV infection in the United States - 2014" (PDF). Centers for Disease Control and Prevention (CDC). Archived from the original (PDF) on 11 April 2018. Retrieved 15 December 2017.
- "Harm Reduction". World Health Organization (WHO). Retrieved 30 July 2020.
- WHO implementation tool for pre-exposure prophylaxis (PrEP) of HIV infection: module 6: pharmacists (Report). World Health Organization (WHO). July 2017. hdl:10665/258509. WHO/HIV/2017.27 License: CC BY-NC-SA 3.0 IGO.
- "FDA approves second drug to prevent HIV infection as part of ongoing efforts to end the HIV epidemic". U.S. Food and Drug Administration (FDA) (Press release). 3 October 2019. Archived from the original on 10 October 2019. Retrieved 10 October 2019.

- "Effectiveness of Prevention Strategies to Reduce the Risk of Acquiring or Transmitting HIV". Centers for Disease Control and Prevention (CDC). 12 November 2019. Archived from the original on 10 December 2019. Retrieved 9 December 2019.
- "National Policies and Guidelines for PrEP". PrEP Watch. Retrieved 5 December 2017.
- Riddell J, Amico KR, Mayer KH (March 2018). "HIV Preexposure Prophylaxis: A Review". JAMA. 319 (12): 1261–1268. doi:10.1001/jama.2018.1917. PMID 29584848. S2CID 205096939.
- "Pre-Exposure Prophylaxis (PrEP) | HIV Risk and Prevention | HIV/AIDS | CDC". www.cdc.gov. 4 June 2020. Retrieved 30 July 2020.
- Ryan B (16 February 2017). "PrEP Fails in a Third Man, But This Time HIV Drug Resistance Is Not to Blame". Poz. Retrieved 15 December 2017.
- Daar ES, Little S, Pitt J, Santangelo J, Ho P, Harawa N, et al. (January 2001). "Diagnosis of primary HIV-1 infection. Los Angeles County Primary HIV Infection Recruitment Network". Annals of Internal Medicine. 134 (1): 25–9. doi:10.7326/0003-4819-134-1-200101020-00010. PMID 11187417. S2CID 34714025.
- "Pre-exposure Prophylaxis for the Prevention of HIV Infection in the United State – 2017 Update Clinical Practice Guideline" (PDF). Centers for Disease Control and Prevention.
- Chou R, Evans C, Hoverman A, Sun C, Dana T, Bougatsos C, et al. (June 2019). "Preexposure Prophylaxis for the Prevention of HIV Infection: Evidence Report and Systematic Review for the US Preventive Services Task Force". JAMA. 321 (22): 2214–2230. doi:10.1001/jama.2019.2591. PMID 31184746.
- Desai M, Field N, Grant R, McCormack S (December 2017). "Recent advances in pre-exposure prophylaxis for HIV". BMJ. 359: j5011. doi:10.1136/bmj.j5011. PMC 6020995. PMID 29229609.
- What's the 2+1+1? Event-driven oral pre-exposure prophylaxis to prevent HIV for men who have sex with men: Update to WHO's recommendation on oral PrEP. Geneva: World Health Organization; 2019 (WHO/CDS/HIV/19.8). Licence: CC BY-NC-SA 3.0 IGO.
- "Preventing HIV During Pregnancy And Breastfeeding in the Context of PrEP". WHO Technical Brief: 16. 2017.
- "Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection". World Health Organization.
- Hodges-Mameletzis I, Fonner VA, Dalal S, Mugo N, Msimanga-Radebe B, Baggaley R (August 2019). "Pre-Exposure Prophylaxis for HIV Prevention in Women: Current Status and Future Directions". Drugs. 79 (12): 1263–1276. doi:10.1007/s40265-019-01143-8. PMID 31309457. S2CID 196811170.
- "Truvada- emtricitabine and tenofovir disoproxil fumarate tablet, film coated". DailyMed. Retrieved 9 December 2019.
- "Descovy- emtricitabine and tenofovir alafenamide tablet". DailyMed. Retrieved 3 August 2020.
- Celum CL (December 2011). "HIV preexposure prophylaxis: new data and potential use". Topics in Antiviral Medicine. 19 (5): 181–5. PMC 6148898. PMID 22298887.
- Marcus JL, Hurley LB, Hare CB, Nguyen DP, Phengrasamy T, Silverberg MJ, et al. (December 2016). "Preexposure Prophylaxis for HIV Prevention in a Large Integrated Health Care System: Adherence, Renal Safety, and Discontinuation". Journal of Acquired Immune Deficiency Syndromes. 73 (5): 540–546. doi:10.1097/QAI.0000000000001129. PMC 5424697. PMID 27851714.
- Ascher SB, Scherzer R, Estrella MM, Shigenaga J, Spaulding KA, Glidden DV, et al. (April 2020). "HIV preexposure prophylaxis with tenofovir disoproxil fumarate/emtricitabine and changes in kidney function and tubular health". Aids. 34 (5): 699–706. doi:10.1097/QAD.0000000000002456. PMC 7071971. PMID 31794523.
- "New research at CROI 2016: How PrEP changes kidney function". San Francisco AIDS Foundation. 8 March 2016. Retrieved 3 August 2020.
- Tetteh RA, Yankey BA, Nartey ET, Lartey M, Leufkens HG, Dodoo AN (April 2017). "Pre-Exposure Prophylaxis for HIV Prevention: Safety Concerns". Drug Safety. 40 (4): 273–283. doi:10.1007/s40264-017-0505-6. PMC 5362649. PMID 28130774.
- 41 HIV and PrEP Patients File California Personal Injury Lawsuit Over Gilead's TDF-Based Drugs; 11 April 2019.
- "AHF Calls on Gilead to Set Up $10 Billion Fund for Victims Harmed by its TDF-based Drugs". AIDS Healthcare Foundation (AHF). 16 July 2019. Retrieved 10 December 2019.
- A question of timing: A lawsuit claims Gilead Sciences could have developed a less-harmful version of its HIV treatment sooner. 29 May 2016.
- Grigsby IF, Pham L, Mansky LM, Gopalakrishnan R, Carlson AE, Mansky KC (March 2010). "Tenofovir treatment of primary osteoblasts alters gene expression profiles: implications for bone mineral density loss". Biochemical and Biophysical Research Communications. 394 (1): 48–53. doi:10.1016/j.bbrc.2010.02.080. PMC 2847063. PMID 20171173.
- Kasonde M, Niska RW, Rose C, Henderson FL, Segolodi TM, Turner K, et al. (13 March 2014). "Bone mineral density changes among HIV-uninfected young adults in a randomised trial of pre-exposure prophylaxis with tenofovir-emtricitabine or placebo in Botswana". PLOS ONE. 9 (3): e90111. Bibcode:2014PLoSO...990111K. doi:10.1371/journal.pone.0090111. PMC 3953113. PMID 24625530.
- "Changes to Your Face and Body (Lipodystrophy & Wasting)". Poz. Retrieved 16 February 2018.
- "PrEP does not raise lipids or alter body fat, safety study finds". Retrieved 16 February 2018.
- "Truvada as HIV PrEP not associated with net fat increase". www.healio.com. Retrieved 16 February 2018.
- "Resource: Side-by-side comparison: Truvada and Descovy for PrEP". San Francisco AIDS Foundation. Retrieved 3 August 2020.
- Gilead. "U.S. Food and Drug Administration Approves Gilead's Truvada for Reducing the Risk of Acquiring HIV". Gilead. Retrieved 15 December 2017.
- "Guidance on oral pre-exposure prophylaxis (PrEP) for serodiscordant couples, men and transgender women who have sex with men at high risk of HIV: recommendations for use in the context of demonstration projects" (PDF). World Health Organization (WHO). July 2012.
- "Policy brief: Consolidated guidelines on HIV prevention, diagnosis, treatment and care for key populations, 2014" (PDF). World Health Organization (WHO). July 2014.
- "WHO expands recommendation on oral pre-exposure prophylaxis of HIV infection (PrEP)" (PDF). World Health Organization (WHO). November 2015. Retrieved 18 December 2015.
- "Korea has just approved PrEP but who can afford it at that price?". Gay Star News. 21 February 2018.
- "Norway becomes first country to offer free PrEP - Star Observer". starobserver.com.au. Retrieved 12 January 2017.
- "Pre-Exposure Prophylaxis (PrEP)". AFAO.org.au. Australian Federation of AIDS Organizations. Retrieved 15 December 2017.
- "Canada and Israel OK Truvada as PrEP to Prevent HIV". Poz. 1 March 2016. Retrieved 12 January 2017.
- Brooks M (22 July 2016). "Truvada Recommended as First Drug for HIV PrEP in Europe". Medscape. Retrieved 15 December 2017.
- "First medicine for HIV pre-exposure prophylaxis recommended for approval in the EU". European Medicines Agency (EMA) (Press release). 22 July 2016. Retrieved 12 January 2017.
- Gilead Sciences Policy Position. "Pre-Exposure Prophylaxis (PrEP) for HIV Prevention" (PDF). Gilead Sciences. Retrieved 15 December 2017.
- "HIV prevention drug Truvada to be publicly funded in New Zealand". Retrieved 7 February 2018.
- "PrEP". Australian Federation of AIDS Organisations. Retrieved 31 July 2020.
- "Truvada for HIV PrEP: How Much It Costs and How to Save - GoodRx". The GoodRx Prescription Savings Blog. 29 August 2018. Retrieved 4 August 2020.
- Nelson, Gary (22 March 2017). "Truvada". Positively Aware. Retrieved 4 August 2020.
- "Generic HIV prevention drug coming in 2020, Gilead says". NBC News. Retrieved 4 August 2020.
- Straube, Trenton (9 May 2019). "Generic PrEP to Arrive in September 2020, but Will Big Savings Follow?". POZ. Retrieved 4 August 2020.
- "Truvada for HIV PrEP: How Much It Costs and How to Save - GoodRx". The GoodRx Prescription Savings Blog. 29 August 2018. Retrieved 4 August 2020.
- "Gilead Advancing Access® Co-pay Coupon Program". www.gileadadvancingaccess.com. Retrieved 4 August 2020.
- McNeil Jr DG (3 December 2019). "200,000 Uninsured Americans to Get Free H.I.V.-Prevention Drugs". The New York Times. Retrieved 10 December 2019.
- "Pre-Exposure Prophylaxis". HIV.gov. 2019. Retrieved 3 August 2020.
- "NPIN PrEP Provider Data and Locator Widget". Centers for Disease Control and Prevention.
- "Bill Text - SB-159 HIV: preexposure and postexposure prophylaxis". leginfo.legislature.ca.gov. Retrieved 31 July 2020.
- "California Makes PrEP and PEP Available Without Prescription". www.advocate.com. 7 October 2019. Retrieved 31 July 2020.
- New York State Department of Public Health. "Ending the AIDS Epidemic in New York State". New York State Department of Public Health. Retrieved 15 December 2017.
- "About HIV and San Francisco". Getting to Zero. San Francisco Department of Public Health. Retrieved 15 December 2017.
- Allday E (15 September 2017). "Aggressive prevention pays off as new HIV infections in SF hit a record low". San Francisco Chronicle. Retrieved 15 December 2017.
- Gay Men's Health Crisis (8 August 2016). "GMHC Launches PrEP Ad Campaign in New York City Bus Shelters". Gay Men's Health Crisis. Retrieved 15 December 2017.
- Simmons-Duffin S. "PrEP Campaign Aims To Block HIV Infection And Save Lives In D.C." Washington Post. Retrieved 31 July 2020.
- "Getting To Zero MA – Welcome to Zero HIV Stigma, Zero HIV Deaths, Zero HIV Infections". www.gettingtozeroma.org. Retrieved 3 August 2020.
- "Getting to Zero CT – Zero HIV Infections. Zero HIV Stigma. Zero HIV Deaths". Retrieved 3 August 2020.
- "Home". gtzillinois.hiv. Retrieved 3 August 2020.
- "Getting to Zero: Silicon Valley | Santa Clara County". Getting to Zero Silicon Valley. Retrieved 3 August 2020.
- "Getting To Zero | Eliminate all new HIV infections in San Diego County within 10 years". Getting To Zero. Retrieved 3 August 2020.
- Johnson, S. R. (30 November 2018). Clinicians warn HIV prevention drug use can lead to risky behavior. Retrieved 10 October 2019, from https://www.modernhealthcare.com/article/20181130/TRANSFORMATION01/181139992/clinicians-warn-hiv-prevention-drug-use-can-lead-to-risky-behavior.
- Broder PhD, M. (n.d.). Does PrEP Lead to Riskier Behavior? Retrieved 10 October 2019, from https://www.medpagetoday.com/resource-centers/contemporary-hiv-prevention/does-prep-lead-riskier-behavior/1179.
- Pre-exposure prophylaxis may increase risky behaviour when introduced, study finds BMJ 2018; 361 doi: https://doi.org/10.1136/bmj.k2514 (Published 6 June 2018) Retrieved 10 October 2019 from https://www.bmj.com/content/361/bmj.k2514
- Glazek C (26 April 2017). "The C.E.O. of H.I.V." The New York Times Magazine. Retrieved 15 December 2017.
- Cairns G (22 February 2017). "STI rates in PrEP users very high, but evidence that PrEP increases them is inconclusive". AIDSMap.com. Retrieved 15 December 2017.
- Highleyman L (24 June 2016). "PrEP use is rising fast in US, but large racial disparities remain". AIDSMap.org. Retrieved 15 December 2017.
- Gallagher J (3 August 2017). "Prep: HIV 'game-changer' to reach NHS in England from September". BBC News Online. Retrieved 15 December 2017.
- Holt M, Lea T, Mao L, Kolstee J, Zablotska I, Duck T, et al. (August 2018). "Community-level changes in condom use and uptake of HIV pre-exposure prophylaxis by gay and bisexual men in Melbourne and Sydney, Australia: results of repeated behavioural surveillance in 2013-17". The Lancet. HIV. 5 (8): e448–e456. doi:10.1016/S2352-3018(18)30072-9. PMID 29885813.
- Duran D (12 November 2012). "Truvada Whores?". HuffPost. Retrieved 27 February 2020.
- Schubert K (2019), "The Democratic Biopolitics of PrEP", in Gerhards H, Braun K (eds.), Biopolitiken – Regierungen des Lebens heute, Politologische Aufklärung – konstruktivistische Perspektiven (in German), Springer Fachmedien Wiesbaden, pp. 121–153, doi:10.1007/978-3-658-25769-9_5, ISBN 978-3-658-25768-2
- "Increasing Access to HIV Prevention Medication | Healthforce Center". healthforce.ucsf.edu. Retrieved 3 August 2020.
- Koechlin FM, Fonner VA, Dalglish SL, O'Reilly KR, Baggaley R, Grant RM, et al. (May 2017). "Values and Preferences on the Use of Oral Pre-exposure Prophylaxis (PrEP) for HIV Prevention Among Multiple Populations: A Systematic Review of the Literature". AIDS and Behavior. 21 (5): 1325–1335. doi:10.1007/s10461-016-1627-z. PMC 5378753. PMID 27900502.
- Baral SD, Poteat T, Strömdahl S, Wirtz AL, Guadamuz TE, Beyrer C (March 2013). "Worldwide burden of HIV in transgender women: a systematic review and meta-analysis". The Lancet. Infectious Diseases. 13 (3): 214–22. doi:10.1016/S1473-3099(12)70315-8. PMID 23260128.
- Pacífico de Carvalho N, Mendicino CC, Cândido RC, Alecrim DJ, Menezes de Pádua CA (October 2019). "HIV pre-exposure prophylaxis (PrEP) awareness and acceptability among trans women: a review". AIDS Care. 31 (10): 1234–1240. doi:10.1080/09540121.2019.1612014. PMID 31043069. S2CID 143425925.
- Mayer KH, Allan-Blitz LT (December 2019). "PrEP 1.0 and Beyond: Optimizing a Biobehavioral Intervention". Journal of Acquired Immune Deficiency Syndromes. 82 Suppl 2: S113–S117. doi:10.1097/QAI.0000000000002169. PMC 6830954. PMID 31658197.
- Denton PW, Estes JD, Sun Z, Othieno FA, Wei BL, Wege AK, et al. (January 2008). "Antiretroviral pre-exposure prophylaxis prevents vaginal transmission of HIV-1 in humanized BLT mice". PLOS Medicine. 5 (1): e16. doi:10.1371/journal.pmed.0050016. PMC 2194746. PMID 18198941.
- Grant RM, Lama JR, Anderson PL, McMahan V, Liu AY, Vargas L, et al. (December 2010). "Preexposure chemoprophylaxis for HIV prevention in men who have sex with men". The New England Journal of Medicine. 363 (27): 2587–99. doi:10.1056/NEJMoa1011205. PMC 3079639. PMID 21091279.
- "PrEP: PK Modeling of Daily TDF/FTC (Truvada) Provides Close to 100% Protection Against HIV Infection". TheBodyPRO.com. Retrieved 28 February 2015.
- Heitz D (23 February 2016). "The Possibility of PrEP that's Not Truvada". HIVEqual. Retrieved 15 December 2017.
- Heitz D (19 October 2015). "PrEP You Don't Swallow: The Future of Anal HIV Prevention". HIVEqual.com. Retrieved 15 December 2017.
- Andrei G, Lisco A, Vanpouille C, Introini A, Balestra E, van den Oord J, et al. (October 2011). "Topical tenofovir, a microbicide effective against HIV, inhibits herpes simplex virus-2 replication". Cell Host & Microbe. 10 (4): 379–89. doi:10.1016/j.chom.2011.08.015. PMC 3201796. PMID 22018238.
- Mansoor LE, Abdool Karim Q, Yende-Zuma N, MacQueen KM, Baxter C, Madlala BT, et al. (May 2014). "Adherence in the CAPRISA 004 tenofovir gel microbicide trial". AIDS and Behavior. 18 (5): 811–9. doi:10.1007/s10461-014-0751-x. PMC 4017080. PMID 24643315.
- "Adherence Indicators and PrEP Drug Levels in the iPrEx Study" (PDF). Archived from the original (PDF) on 4 March 2016. Retrieved 23 December 2015.
- Celum C, Baeten JM (February 2012). "Tenofovir-based pre-exposure prophylaxis for HIV prevention: evolving evidence". Current Opinion in Infectious Diseases. 25 (1): 51–7. doi:10.1097/QCO.0b013e32834ef5ef. PMC 3266126. PMID 22156901.
- Baeten JM, Donnell D, Ndase P, Mugo NR, Campbell JD, Wangisi J, et al. (August 2012). "Antiretroviral prophylaxis for HIV prevention in heterosexual men and women". The New England Journal of Medicine. 367 (5): 399–410. doi:10.1056/NEJMoa1108524. PMC 3770474. PMID 22784037.
- Thigpen MC, Kebaabetswe PM, Paxton LA, Smith DK, Rose CE, Segolodi TM, et al. (August 2012). "Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana". The New England Journal of Medicine. 367 (5): 423–34. doi:10.1056/NEJMoa1110711. PMID 22784038.
- "Top Stories: Poor Adherence Crippled PrEP Efficacy in Women's Study - by Tim Horn". aidsmeds.com. Retrieved 23 December 2015.
- "Top Stories: Failed VOICE PrEP Trial Failed to Preempt Lies About Adherence". aidsmeds.com. Retrieved 23 December 2015.
- Choopanya K, Martin M, Suntharasamai P, Sangkum U, Mock PA, Leethochawalit M, et al. (June 2013). "Antiretroviral prophylaxis for HIV infection in injecting drug users in Bangkok, Thailand (the Bangkok Tenofovir Study): a randomised, double-blind, placebo-controlled phase 3 trial". Lancet. 381 (9883): 2083–90. doi:10.1016/S0140-6736(13)61127-7. PMID 23769234. S2CID 5831642.
- "Bangkok Tenofovir Study: PrEP for HIV prevention among people who inject drugs" (PDF). Centers for Disease Control and Prevention (CDC). Retrieved 23 December 2015.
- Molina JM, Capitant C, Spire B, Pialoux G, Cotte L, Charreau I, et al. (December 2015). "On-Demand Preexposure Prophylaxis in Men at High Risk for HIV-1 Infection". The New England Journal of Medicine. 373 (23): 2237–46. doi:10.1056/NEJMoa1506273. PMID 26624850.
- Gilles Pialoux. "Ipergay: La Prep "à la demande", ça marche fort (quand on la prend)". Cite journal requires
|journal=(help) - Dolling DI, Desai M, McOwan A, Gilson R, Clarke A, Fisher M, et al. (March 2016). "An analysis of baseline data from the PROUD study: an open-label randomised trial of pre-exposure prophylaxis". Trials. 17: 163. doi:10.1186/s13063-016-1286-4. PMC 4806447. PMID 27013513.
- "HPTN 083 FAQ" (PDF). HPTN. 17 May 2020.
- "DISCOVER Trial Factsheet". AVAC. 6 December 2016. Retrieved 13 February 2019.
- Holt M, Lea T, Mao L, Kolstee J, Zablotska I, Duck T, et al. (August 2018). "Community-level changes in condom use and uptake of HIV pre-exposure prophylaxis by gay and bisexual men in Melbourne and Sydney, Australia: results of repeated behavioural surveillance in 2013-17". The Lancet. HIV. 5 (8): e448–e456. doi:10.1016/s2352-3018(18)30072-9. PMID 29885813.
- "Does PrEP Use Lead to Higher STI Rates Among Gay and Bi Men?". Poz. 2 September 2016. Retrieved 23 July 2018.
- "STD Facts - Syphilis (Detailed)". Centers for Disease Control and Prevention (CDC). 23 September 2019.
- "Update to Gonorrhea Treatment Guidelines" (PDF). U.S. Centers for Disease Control and Prevention.
- "Chlamydia Treatment and Care". Centers for Disease Control and Prevention (CDC). 11 January 2019.
- Dall C (4 September 2018). "Experts brace for more super-resistant gonorrhea". CIDRAP News - Center for Infectious Disease Research and Policy. University of Minnesota.
- Freeborn K, Portillo CJ (September 2018). "Does pre-exposure prophylaxis for HIV prevention in men who have sex with men change risk behaviour? A systematic review". Journal of Clinical Nursing. 27 (17–18): 3254–3265. doi:10.1111/jocn.13990. PMC 5797507. PMID 28771856.
- Hodges-Mameletzis I, Fonner VA, Dalal S, Mugo N, Msimanga-Radebe B, Baggaley R (August 2019). "Pre-Exposure Prophylaxis for HIV Prevention in Women: Current Status and Future Directions". Drugs. 79 (12): 1263–1276. doi:10.1007/s40265-019-01143-8. PMID 31309457. S2CID 196811170.
Further reading
- Kuhar DT, Henderson DK, Struble KA, Heneine W, Thomas V, Cheever LW, et al. (September 2013). "Updated US Public Health Service guidelines for the management of occupational exposures to human immunodeficiency virus and recommendations for postexposure prophylaxis". Infection Control and Hospital Epidemiology. 34 (9): 875–92. doi:10.1086/672271. PMID 23917901. 20711.
- Lange JM (September 2005). "We must not let protestors derail trials of pre-exposure prophylaxis for HIV". PLOS Medicine. 2 (9): e248. doi:10.1371/journal.pmed.0020248. PMC 1176241. PMID 16008501.
- Singh JA, Mills EJ (September 2005). "The abandoned trials of pre-exposure prophylaxis for HIV: what went wrong?". PLOS Medicine. 2 (9): e234. doi:10.1371/journal.pmed.0020234. PMC 1176237. PMID 16008507.
External links
- PrEPWatch PrEP Watch homepage
- CDC Pre-Exposure Prophylaxis (PrEP), Centers for Disease Control and Prevention (CDC)
- CM Mediclinic Thailand What is PrEP?
- The Game Changer Project Prep HIV
- "Oral PrEP Tool app". World Health Organization (WHO).
| Authority control |
|
|---|