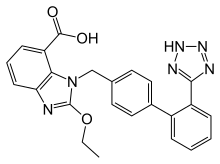
Candesartan
Candesartan is an angiotensin receptor blocker used mainly for the treatment of high blood pressure and congestive heart failure.
 | |
| Clinical data | |
|---|---|
| Pronunciation | /ˌkændɪˈsɑːrtən/ |
| Trade names | Atacand, others |
| Other names | Candesartan cilexetil |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a601033 |
| Pregnancy category |
|
| Routes of administration | By mouth |
| ATC code | |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | 15% (candesartan cilexetil) |
| Metabolism | Candesartan cilexetil: intestinal wall; candesartan: hepatic (CYP2C9) |
| Elimination half-life | 9 hours |
| Excretion | Kidney 33%, faecal 67% |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| CompTox Dashboard (EPA) | |
| ECHA InfoCard | 100.132.654 |
| Chemical and physical data | |
| Formula | C24H20N6O3 |
| Molar mass | 440.463 g·mol−1 |
| 3D model (JSmol) | |
| |
| |
| | |
It was patented in 1990 and approved for medical use in 1997.[1]
Medical uses
Hypertension
As with other angiotensin II receptor antagonists, candesartan is indicated for the treatment of hypertension.[2] Candesartan has an additive hypertensive effect when combined with a diuretic, such as chlortalidone. It is available in a combination formulation with a low dose of the thiazide diuretic hydrochlorothiazide. Candesartan/hydrochlorothiazide combination preparations are marketed under various trade names including Atacand HCT, Hytacand, Blopress Plus, Advantec and Ratacand Plus.
Congestive heart failure
Results from the CHARM study (early 2000s) demonstrated the morbidity and mortality reduction benefits of candesartan therapy in congestive heart failure.[3]
Prehypertension
In a four-year randomized controlled trial, candesartan was compared to placebo to see whether it could prevent or postpone the development of full-blown hypertension in people with so-called prehypertension. During the first two years of the trial, half of participants were given candesartan, and the others received placebo; candesartan reduced the risk of developing hypertension by nearly two-thirds during this period. In the last two years of the study, all participants were switched to placebo. By the end of the study, candesartan had significantly reduced the risk of hypertension, by more than 15%. Serious adverse effects were more common among participants receiving placebo than in those given candesartan.[4]
Prevention of atrial fibrillation
A meta-analysis found that candesartan reduces risk of atrial fibrillation in persons with systolic left ventricular dysfunction or with left ventricular hypertrophy.[5] (This was also true of other angiotensin receptor blockers and of angiotensin converting enzyme inhibitors).
Diabetic retinopathy
Use of antihypertensive drugs, including candesartan, in patients with diabetic retinopathy, has been demonstrated to slow the progression of diabetic retinopathy.[6]
Adverse effects
As with other drugs that inhibit the renin–angiotensin system, if candesartan is taken by pregnant women during the second or third trimester, it can cause injury and in some cases, death of the developing fetus. Symptomatic hypotension may occur in people who take candesartan and are volume-depleted or salt-depleted, as can also occur when diuretics are coadministered. Reduction in renal glomerular filtration rate may occur; people with renal artery stenosis may be at higher risk. Hyperkalemia may occur; people who are also taking spironolactone or eplerenone may be at higher risk.[2]
Anemia may occur, due to inhibition of the renin–angiotensin system.[9]
As with other angiotensin receptor blockers, candesartan can rarely cause severe liver injury.[10]
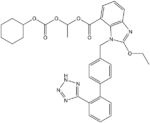
Chemistry and pharmacokinetics
Candesartan is marketed as the cyclohexyl 1-hydroxyethyl carbonate (cilexetil) ester, known as candesartan cilexetil. Candesartan cilexetil is metabolised completely by esterases in the intestinal wall during absorption to the active candesartan moieity.
The use of a prodrug form increases the bioavailability of candesartan. Despite this, absolute bioavailability is relatively poor at 15% (candesartan cilexetil tablets) to 40% (candesartan cilexetil solution). Its IC50 is 15 μg/kg.
History
The compound known as TCV-116 (candesartan) was studied by Japanese scientists using standard laboratory rats. Animal studies were published showing the effectiveness of the compound in 1992–1993, with a pilot study on humans published in the summer of 1993.[11][12]
Names
The prodrug candesartan cilexetil is marketed by AstraZeneca and Takeda Pharmaceuticals, commonly under the trade names Blopress, Atacand, Amias, and Ratacand. It is available in generic form.
References
- Fischer, Jnos; Ganellin, C. Robin (2006). Analogue-based Drug Discovery. John Wiley & Sons. p. 471. ISBN 9783527607495.
- "Candesartan label" (PDF). FDA. February 2016. For label updates see FDA index page for IND 020838
- Pfeffer M, Swedberg K, Granger C, Held P, McMurray J, Michelson E, Olofsson B, Ostergren J, Yusuf S, Pocock S (2003). "Effects of candesartan on mortality and morbidity in patients with chronic heart failure: the CHARM-Overall programme". Lancet. 362 (9386): 759–66. doi:10.1016/S0140-6736(03)14282-1. PMID 13678868.
- Julius S, Nesbitt SD, Egan BM, et al. (July 2006). "Feasibility of treating prehypertension with an angiotensin-receptor blocker". New England Journal of Medicine. 354 (16): 1685–97. doi:10.1056/NEJMoa060838. PMID 16537662.
- Healey, Jeff S., Adrian Baranchuk, Eugene Crystal, Carlos A. Morillo, Michael Garfinkle, Salim Yusuf, and Stuart J. Connolly. "Prevention of atrial fibrillation with angiotensin-converting enzyme inhibitors and angiotensin receptor blockers: a meta-analysis." Journal of the American College of Cardiology 45, no. 11 (2005): 1832-1839.
- Elkjaer AS, Lynge SK, Grauslund J (February 2020). "Evidence and indications for systemic treatment in diabetic retinopathy: a systematic review". Acta Ophthalmol. doi:10.1111/aos.14377. PMID 32100477.
- Dorosch T, Ganzer CA, Lin M, Seifan A (September 2019). "Efficacy of Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers in the Preventative Treatment of Episodic Migraine in Adults". Curr Pain Headache Rep. 23 (11): 85. doi:10.1007/s11916-019-0823-8. PMID 31515634.
- Cernes R, Mashavi M, Zimlichman R (2011). "Differential clinical profile of candesartan compared to other angiotensin receptor blockers". Vasc Health Risk Manag. 7: 749–59. doi:10.2147/VHRM.S22591. PMC 3253768. PMID 22241949.
- Cheungpasitporn, W; Thongprayoon, C; Chiasakul, T; Korpaisarn, S; Erickson, SB (November 2015). "Renin-angiotensin system inhibitors linked to anemia: a systematic review and meta-analysis". QJM : Monthly Journal of the Association of Physicians. 108 (11): 879–84. doi:10.1093/qjmed/hcv049. PMID 25697787.

- Patti R, Sinha A, Sharma S, Yoon TS, Kupfer Y (May 2019). "Losartan-induced Severe Hepatic Injury: A Case Report and Literature Review". Cureus. 11 (5): e4769. doi:10.7759/cureus.4769. PMC 6663042. PMID 31363450.
- Mizuno, K.; et al. (1992). "Hypotensive activity of TCV-116, a newly developed angiotensin II receptor antagonist, in spontaneously hypertensive rats". Life Sci. 51 (20): PL183-187. doi:10.1016/0024-3205(92)90627-2. PMID 1435062.
- Ogihara, T.; et al. (Jul–Aug 1993). "Pilot study of a new angiotensin II receptor antagonist, TCV-116: effects of a single oral dose on blood pressure in patients with essential hypertension". Clin. Ther. 15 (4): 684–91. PMID 8221818.