Tumefactive multiple sclerosis
Tumefactive multiple sclerosis is a condition in which the central nervous system of a person has multiple demyelinating lesions with atypical characteristics for those of standard multiple sclerosis (MS). It is called tumefactive as the lesions are "tumor-like" and they mimic tumors clinically, radiologically and sometimes pathologically.[1]
| Tumefactive multiple sclerosis | |
|---|---|
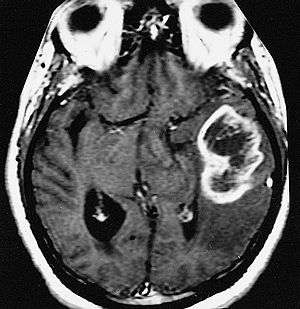 | |
| An example of a ring-enhancement around a lesion in gliobastoma. In tumefactive multiple sclerosis, the ring-enhancement is open, not forming a complete ring. |
These atypical lesion characteristics include a large intracranial lesion of size greater than 2.0 cm with a mass effect, edema and an open ring enhancement. A mass effect is the effect of a mass on its surroundings, for example, exerting pressure on the surrounding brain matter. Edema is the build-up of fluid within the brain tissue. Usually, the ring enhancement is directed toward the cortical surface.[2] The tumefactive lesion may mimic a malignant glioma or cerebral abscess causing complications during the diagnosis of tumefactive MS. T2-hypointense rim and incomplete ring enhancement of the lesions on post-gadolinium T1- weighted imaging on brain MRI enable accurate diagnosis of TDL[3]
Normally a tumefactive demyelinating lesion appears together with smaller disseminated lesions separated in time and space, yielding a diagnosis of Multiple Sclerosis. Hence the name "tumefactive multiple sclerosis". When the demyelinating lesion appears alone it has been termed solitary sclerosis.[4][5][6] These cases belong to a multiple sclerosis borderline and there is currently no universal agreement on how they should be considered.
Tumefactive multiple sclerosis is a demyelinating and inflammatory disease. Myelination of the axons are highly important for signalling as this improves the speed of conduction of action potentials from one axon to the next. This is done through the formation of high-resistance, low-conductance myelin sheaths around the axons by specific cells called oligodendrocytes. As such, the demyelination process affects the communication between neurons and this consequently affects the neural pathways they control. Depending on where the demyelination takes place and its severity, patients with tumefactive MS have different clinical symptoms.[7]
Signs and symptoms
Symptoms of standard MS consist of both sensory and motor symptoms. The more common symptoms include spasticity, visual loss, difficulty in walking and paresthesia which is a feeling of tickling or numbness of the skin.[8] but symptoms of tumefactive MS are not so clear. They often mimic a variety of other diseases including ischemic stroke, peroneal nerve palsy and intracranial neurologic disease.
Subjects have been reported to suffer from a decreased motor control resulting in a ‘foot drop’,[9] or significantly reduced leg movement.[10] In other cases closer mimicking strokes, subjects may suffer from confusion, dizziness, and weakness in one side of the face.[11] Symptoms also can mimic a neoplasm with symptoms such as headaches, aphasia, and/ or seizures.[13]
There are some differences with normal MS symptoms.
Spasticity is not as prevalent in tumefactive cases, because in standard MS it is caused by demyelination or inflammation in the motor areas of the brain or the spinal cord.[8] This upper motor neuron syndrome appears when motor control of skeletal muscles is affected due to damage to the efferent motor pathways. Spasticity is an involuntary muscle movement like an exaggerated stretch reflex, which is when a muscle overcompensates and contracts too much in response to the muscle being stretched. It is believed that spasticity is the result of the lack of inhibitory control on the muscles, an effect of neuronal damage.[12]
Visual loss or disturbances are also different. In standard MS, they are a result of inflammation of the optic nerve, known as optic neuritis. The effects of optic neuritis can be loss of color perception and worsening vision. Vision loss usually starts off centrally in one eye and may lead to complete loss of vision after a period of time.[8]
The possible cognitive dysfunction is also rare in tumefactive cases. MS patients may show signs of cognitive impairment where there is a reduction in the speed of information processing, a weaker short-term memory and a difficulty in learning new concepts.[13] This cognitive impairment is associated with the loss of brain tissue, known as brain atrophy which is a result of the demyelination process in MS.[14]
About fatigue: most MS patients experience fatigue and this could be a direct result of the disease, depression or sleep disturbances due to MS. It is not clearly understood how MS results in physical fatigue but it is known that the repetitive usage of the same neural pathways results in nerve fiber fatigue that could cause neurological symptoms. Such repeated usage of neural pathways include continuous reading which may result in temporary vision failure.[8]
Evolution
Some reports indicate that an initial tumefactive lesion can evolve to various pathological entities: multiple sclerosis (the most common), Balo's concentric sclerosis, Schilder's disease and acute disseminated encephalomyelitis[15]
Course
Usually tumefactive demyelination is monophasic, but cases with recurrence have been reported[16]
Cause
The pathology of the tumefactive demyelinating lesion (TDL) is heterogeneous.[17] There are several conditions can produce tumefactive lesions. This is known because in some special cases the etiology can be identified. For example, there are some cases of NMO, misidentified as MS and treated with interferon-beta by mistake. Some of these patients developed tumefactive lesions.[18][19] Anyway, it is important to have into account that NMO itself can also produce them[20][21]
Some other cases have been found related to viral infection,[22] some others related to NMOSD,[23] others could be paraneoplastic,[24][25] Also some cases could be related to hormonal treatments[26]
Other possible cause are immunomodulatory combinations. In particular, it has been found that switching from standard MS therapies to fingolimod can trigger tumefactive lesions in some MS patients[27][28][29][30] While standard multiple sclerosis process has an autoimmune response after the breach of the blood-brain barrier, in tumefactive MS things do not process in the same way, and demyelinating lesions do not always show antibody damage. Subjects with tumefactive multiple sclerosis display elevated levels of choline (Cho)/creatine ratio and increased lactate which is associated with demylinating diseases. Cases also display oligoclonal bands in the cerebrospinal fluid.[11]
The disease is heterogeneous and the lesions do not always comply with the requirements for multiple sclerosis diagnosis (dissemination in time and space). In these cases it is only possible to speak about tumefactive demyelination (TD).[31]
In general, it is accepted that the two main causes of pseudo-tumoral lesions are Marburg multiple sclerosis and acute disseminated encephalomyelitis (ADEM).[32] Tumefactive demyelination of the spinal cord is rare but it has been reported[33]
Damage is not confined to the demyelinating area. Wallerian degeneration outside the lesions has been reported.[34]
In general, during the acute phase, the plaques of lesions were characterized by massive demyelination with relatively axonal preservation associated with reactive astrocytosis and infiltration of macrophages. In plaques of chronic lesions, demyelinated lesions with relative axonal preservation and sharply defined margins were major findings. And myelin-laden macrophages accumulate at the edges of plaques and stay inactive[35]
Diagnosis
Diagnosis of tumefactive MS is commonly carried out using magnetic resonance imaging (MRI) and proton MR spectroscopy (H-MRS). Diagnosis is difficult as tumefactive MS may mimic the clinical and MRI characteristics of a glioma or a cerebral abscess. However, as compared to tumors and abscesses, tumefactive lesions have an open-ring enhancement as opposed to a complete ring enhancement.[1] Even with this information, multiple imaging technologies have to be used together with biochemical tests for accurate diagnosis of tumefactive MS.[36]
Tumefactive demyelination is distinguished from tumor by the presence of multiple lesions, absence of cortical involvement, and decrease in lesion size or detection of new lesions on serial imaging[37] Tumefactive lesions can appear in the spinal cord, making the diagnosis even more difficult.[38]
Magnetic resonance imaging
MRI diagnosis is based on lesions that are disseminated in time and space, meaning that there are multiple episodes and consisting of more than one area.[39] There are two kinds of MRI used in the diagnosis of tumefactive MS, T1-weighted imaging and T2-weighted imaging. Using T1-weighted imaging, the lesions are displayed with low signal intensity, meaning that the lesions appear darker than the rest of the brain. Using T2-weighted imaging, the lesions appear with high signal intensity, meaning that the lesions appear white and brighter than the rest of the brain. When T1-weighted imaging is contrast-enhanced through the addition of gadolinium, the open ring enhancement can be viewed as a white ring around the lesion.[40] A more specific MRI, Fluid attenuation inversion recovery (FLAIR) MRI show the signal intensity of the brain. Subjects with tumefactive multiple sclerosis may see a reduction of diffusion of the white matter in the affected area of the brain.[11]
Proton MR spectroscopy
Proton (H+) MR spectroscopy (H-MRS) identifies biochemical changes in the brain such as the quantity of metabolic products of neural tissue including choline, creatine, N-acetylaspartate (NAA), mobile lipids and lactic acid.
When demyelination is occurring, there is breakdown of cell membranes resulting in an increase in the level of choline. NAA is specific to neurons and thus, a reduction in NAA concentration indicates neuronal or axonal dysfunction. As such, the levels of choline and NAA can be measured to determine if there is demyelination activity and inflammation in the brain.
Usually, the ratio of choline to NAA is used as biomarker [41] being higher in gliomas than in TDLs or MS lesions[42]
Treatment
Typical tumefactive lesions have been found to be responsive to corticosteroids because of their immunosuppressive and anti-inflammatory properties. They restore the blood-brain barrier and induce cell death of T-cells.[13]
No standard treatment exists, but practitioners seem to apply intravenous corticosteroids, followed by plasmapheresis and cyclophosphamide in non-responsive cases[43] High dose intravenous corticosteroids (methylprednisolone 1 g for 3–5 days) followed by oral tapering hasten clinical and radiological improvement in approximately 80% of patients[44]
Plasmapheresis has been reported to work even in the absence of response to corticosteroids[45]
Disease-modifying agents
Pharmacologic treatments for MS include immunomodulators and immunosuppressants which reduce the frequency and severity of relapses by about 35% and reduce the lesion growth.[46] Unfortunately they are mainly tested for RRMS and its effect in tumefactive lesions is unknown. The main ones are Interferon beta (IFN-beta), Glatiramer acetate and Mitoxantrone
Plasma exchange has been reported to work at least in some cases[47]
Treatment of symptoms
Due to the wide range of symptoms experienced by people with MS, the treatment for each MS patient varies depending on the extent of the symptoms.
Spasticity
The treatment of spasticity ranges from physical activity to medication. Physical activity includes stretching, aerobic exercises and relaxation techniques. Currently, there is little understanding as to why these physical activities aid in relieving spasticity. Medical treatments include baclofen, diazepam and dantrolene which is a muscle-relaxant. Dantrolene has many side effects and as such, it is usually not the first choice in treatment of spasticity. The side effects include dizziness, nausea and weakness.[13]
Fatigue
Fatigue is a common symptom and affects the daily life of individuals with MS. Changes in lifestyle are usually recommended to reduce fatigue. These include taking frequent naps and implementing exercise. MS patients who smoke are also advised to stop. Pharmacological treatment include anti-depressants and caffeine. Aspirin has also been experimented with and from clinical trial data, MS patients preferred using aspirin as compared to the placebo in the test. One hypothesis is that aspirin has an effect on the hypothalamus and can affect the perception of fatigue through altering the release of neurotransmitters and the autonomic responses.[13]
Cognitive dysfunction
There are no approved drugs for the treatment of cognitive dysfunction, however, some treatments have shown an association with improvements in cognitive function. One such treatment is Ginkgo biloba, is a herb commonly used by patients with Alzheimer's disease.[13]
Epidemiology
Approximately 2 million people in the world suffer from multiple sclerosis[48] Tumefactive multiple sclerosis cases make up 1 to 2 of every 1000 multiple sclerosis cases. This means that only around 2000 people in the world suffer of tumefactive MS. Of those cases, there is a higher percentage of females affected than males. The median age of onset is 37 years.[36]
As in general MS, there are differences for gender, ethnicity and geographic location. Based on epidemiological studies, there are about 3 times more female MS patients than male patients, indicating a possibility of an increased risk due to hormones. Among different ethnic groups, MS is the most common among Caucasians and seems to have a greater incidence at latitudes above 40° as compared to at the equator. While these associations have been made, it is still unclear how they result in an increased risk of MS onset.[49]
Solitary sclerosis
Normally a tumefactive demyelinating lesion appears together with smaller disseminated lesions. Hence the name "tumefactive multiple sclerosis". When the demyelinating lesion appears alone it has been termed "solitary sclerosis"
This variant was first proposed (2012) by Mayo Clinic researches.[4] though it was also reported by other groups more or less at the same time.[50][51] It is defined as isolated demyelinating lesions which produce a progressive myelopathy similar to primary progressive MS,[52][53][54] and is currently considered inside the Tumefactive Multiple sclerosis.[5] Some groups have reported some kind of response of this variant to biotin[55]
solitary pontine lesion
Syndrome consisting in solitary lesions uniformly located along the trigeminal pontine pathway, producing trigeminal neuralgia (TN). They present similar clinical features than MS-TN but with a single pontine lesion.[56]
MOG antibody‐associated demyelinating pseudotumor
- Main article: anti-MOG associated encephalomyelitis
Some anti-MOG cases satisfy the MS requirements (lesions disseminated in time and space) and are therefore traditionally considered MS cases. After the discovery of the anti-MOG disease this classification is into revision.[57]
See also
- Idiopathic inflammatory demyelinating diseases
- Malignant multiple sclerosis
- Marburg acute multiple sclerosis
References
- Xia L., Lin S., Wang Z., Li S., Xu L., Wu J., Hao S., Gao C. (2009). "Tumefactive demyelinating lesions: nine cases and a review of the literature". Neurosurg Rev. 32 (2): 171–179. doi:10.1007/s10143-009-0185-5. PMID 19172322.CS1 maint: multiple names: authors list (link)
- Kaeser, M. A., Scali, F., Lanzisera, F. P., Bub, G. A., and Kettner, N. W. Tumefactive multiple sclerosis: an uncommon diagnostic challenge. Journal of Chiropractic Medicine 10:29-35 (2011).
- Kilic AK, Kurne AT, Oguz KK, Soylemezoglu F, Karabudak R (2013). "Mass lesions in the brain: tumor or multiple sclerosis? Clinical and imaging characteristics and course from a single reference center" (PDF). Turk Neurosurg. 23 (6): 728–35. doi:10.5137/1019-5149.JTN.7690-12.3 (inactive 2020-05-29). PMID 24310455. Retrieved 19 March 2020.CS1 maint: multiple names: authors list (link)
- Schmalstieg WF, Keegan BM, Weinshenker BG (February 2012). "Solitary sclerosis: progressive myelopathy from solitary demyelinating lesion". Neurology. 78 (8): 540–4. doi:10.1212/WNL.0b013e318247cc8c. PMID 22323754.
- Jiménez Arango JA, Uribe Uribe CS, Toro González G (2013). "Lesser-known myelin-related disorders: Focal tumour-like demyelinating lesions". Neurologia. 30 (2): 97–105. doi:10.1016/j.nrl.2013.06.004. PMID 24094691.
- Kalavakunta, Jagadeesh K.; Tokala, Hemasri; Loehrke, Mark (2011-08-01). "Solitary lesion in magnetic resonance imaging: tumor versus multiple sclerosis". The American Journal of the Medical Sciences. 342 (2): 168. doi:10.1097/MAJ.0b013e318200d247. ISSN 1538-2990. PMID 21799469.
- Moore G. R. W., Esiri M. M. (2011). "The pathology of multiple sclerosis and related disorders". Diagnostic Histopathology. 17 (5): 225–231. doi:10.1016/j.mpdhp.2011.02.001.
- Rudick, R. A. Contemporary Diagnosis and Management of Multiple Sclerosis. Pennsylvania: Handbooks in Health Care Co., 2004. Print.
- Kaeser Martha A., Scali Frank, Lanzisera Frank P., Bub Glenn A., Kettner Norman W. (2011). "Tumefactive multiple sclerosis: an uncommon diagnostic challenge". Journal of Chiropractic Medicine. 10 (1): 29–35. doi:10.1016/j.jcm.2010.08.002. PMC 3110404. PMID 22027206.CS1 maint: multiple names: authors list (link)
- Yamada So, Merrit Yamada Shoko, Nakaguchi Hiroshi, Murakami Mineko, Hoya Katsumi, Matsuno Akira, Yamazaki Kazuto, Ishida Yasuo (2012). "Tumefactive multiple sclerosis requiring emergent biopsy and histological investigation to confirm the diagnosis: a case report". Journal of Medical Case Reports. 6 (9): 104. doi:10.1186/1752-1947-6-104. PMC 3337287. PMID 22483341.CS1 maint: multiple names: authors list (link)
- Yacoub Hussam A., Al-Qudahl Zaid A., Lee Huey-Jen, Baisre Ada, Souayah Nizar (2011). "Tumefactive Multiple Sclerosis presenting as Acute Ischemic Stroke". Journal of Vascular and Interventional Neurology. 4 (2): 21–23. PMC 3317283. PMID 22518267.CS1 maint: multiple names: authors list (link)
- Purves, D., Augustine, G. J., Fitzpatrick, D., Hall, W. C., LaMantia, A. S., and White, L. E. Neuroscience. Sunderland: Sinauer Associates Inc., U.S., 2010. Print.
- Crayton H. J., Rossman H. S. (2006). "Managing the Symptoms of Multiple Sclerosis: A Multimodal Approach". Clinical Therapeutics. 28 (4): 445–460. doi:10.1016/j.clinthera.2006.04.005. PMID 16750459.
- Pelletier J., Suchet L., Witjas T.; et al. (2001). "A longitudinal study of callosal atrophy and interhemispheric dysfunction in relapsing-remitting multiple sclerosis". Arch Neurol. 58 (1): 105–111. doi:10.1001/archneur.58.1.105. PMID 11176943.CS1 maint: multiple names: authors list (link)
- Balloy G et al. Inaugural tumor-like multiple sclerosis: clinical presentation and medium-term outcome in 87 patients. J Neurol. 2018 Jul 27. doi: 10.1007/s00415-018-8984-7
- Jamir Pitton Rissardo,Ana Letícia Fornari Caprara, Management of Recurrent Tumefactive Multiple Sclerosis: Case Report and Literature Review, Asian J Neurosurg. 2018 Jul-Sep; 13(3): 893–896. doi: 10.4103/ajns.AJNS_94_18
- Weinshenker Brian G (2015). "Tumefactive demyelinating lesions: Characteristics of individual lesions, individual patients, or a unique disease entity?". Mult Scler. 21 (13): 1746–1747. doi:10.1177/1352458515603801. PMID 26362899.
- Harmel J, Ringelstein M, Ingwersen J, Mathys C, Goebels N, Hartung HP, Jarius S, Aktas O (Dec 2014). "Interferon-β-related tumefactive brain lesion in a Caucasian patient with neuromyelitis optica and clinical stabilization with tocilizumab". BMC Neurol. 14 (1): 247. doi:10.1186/s12883-014-0247-3. PMC 4301061. PMID 25516429.CS1 maint: multiple names: authors list (link)
- Bomprezzi Roberto, Powers J. Michael (2011). "IFNβ-1b may severely exacerbate Japanese opticspinal MS in neuromyelitis optica spectrum: Japanese optic-spinal MS: Is it MS or neuromyelitis optica and does the answer dictate treatment?". Neurology. 77 (2): 195–196. doi:10.1212/WNL.0b013e318219dde5. PMID 21747078.
- Kazuo Fujihara MD, Misu Tatsuro (2015). "AQP4 in biopsied demyelinating lesions as a diagnostic clue to NMOSD and MS". Neurology. 84 (2): 110–111. doi:10.1212/WNL.0000000000001135. PMID 25503619.
- Ujjawal R; et al. (2016). "Neuromyelitis Optica Spectrum Disorder with Tumefactive Demyelination mimicking Multiple Sclerosis: a rare case". Front. Neurol. 7: 73. doi:10.3389/fneur.2016.00073. PMC 4862986. PMID 27242658.
- Handa Rahul (2014). "Tumefactive demyelination: A rare presentation of HIV" (PDF). Annals of Tropical Medicine and Public Health. 7 (4).
- Ikeda Ken; et al. (2011). "Repeated Non-enhancing Tumefactive Lesions in a Patient with a Neuromyelitis Optica Spectrum Disorder". Internal Medicine. 50 (9): 1061–1064. doi:10.2169/internalmedicine.50.4295. PMID 21532234.
- Broadfoot Jack R (2015). "Paraneoplastic tumefactive demyelination with underlying combined germ cell cancer". Pract Neurol. 15 (6): 451–455. doi:10.1136/practneurol-2015-001146. PMID 26088612.
- Van Haver, Anne-Sophie; Debruyne, Frederik; Sanders, Katrien; Verstappen, Annick (March 2020). "Paraneoplastic tumefactive demyelination in a 47-year-old man with underlying seminoma". Multiple Sclerosis and Related Disorders. 42: 102060. doi:10.1016/j.msard.2020.102060. PMID 32217464.
- Vaknin-Dembinsky; et al. (Jan 2015). "Tumefactive demyelination following in vitro fertilization (IVF)". J Neurol Sci. 348 (1–2): 256–8. doi:10.1016/j.jns.2014.11.016. PMID 25499758.
- Hellmann M.A. (2014). "Tumefactive demyelination and a malignant course in an MS patient during and following fingolimod therapy". Journal of the Neurological Sciences. 344 (1–2): 193–197. doi:10.1016/j.jns.2014.06.013. PMID 25001515.
- Lee YuanKai; et al. (2014). "Tumefactive Multiple Sclerosis in a Patient on Fingolimod". Neurology. 82 (10): 226.
- Harirchian M.H.; et al. (2015). "Emerging Tumefactive MS after switching therapy from Interferon-beta to Fingolimod; a case report". Multiple Sclerosis and Related Disorders. 4 (5): 400–402. doi:10.1016/j.msard.2015.05.007. PMID 26346786.
- Steinhoff Timothy B, Scott Thomas F (2015). "Tumefactive Demyelination with White Matter Necrosis Following Cessation of Natalizumab Treatment". Neurological Cases. 2 (1).
- Masaki; et al. (2014). "Gadolinium enhancement patterns of tumefactive demyelinating lesions: correlations with brain biopsy findings and pathophysiology". Journal of Neurology. 261 (10): 1902–1910. doi:10.1007/s00415-014-7437-1. PMID 25034274.
- Antonella; et al. (2014). "Neuronavigation-guided biopsy for differential diagnosis of pseudotumoral demyelinating brain lesions". Interdisciplinary Neurosurgery. 1 (3): 44–46. doi:10.1016/j.inat.2014.04.002.
- Kantorová E, Marcinek J, Zeleňák K, Kantor K, Michalik J, Sivák Š, Kurča E, Plank L (2015). "Tumefactive demyelination of the spinal cord: a case report". Spinal Cord. 53 (12): 877–880. doi:10.1038/sc.2015.52. PMID 26123208.CS1 maint: multiple names: authors list (link)
- Told A.; et al. (2016). "Hardy et al. Wallerian Degeneration in the Corticospinal Tract Following Tumefactive Demyelination: Conventional and Advanced Magnetic Resonance Imaging". Canadian Journal of Neurological Sciences. 43 (5): 726–727. doi:10.1017/cjn.2016.253. PMID 27417915.
- Sun C, Liu J, Gui Q, Lu D, Qi X (2014). "Analysis of pathological characteristics of acute and chronic cerebral tumefactive demyelinating lesions". Zhonghua Yi Xue Za Zhi. 94 (45): 3557–3561. PMID 25622833.
- Lucchinetti CF, Gavrilova RH, Metz I, Parisi JE, Scheithauer BW, Weigand S, et al. (2008). "Clinical and radiographic spectrum of pathologically confirmed tumefactive multiple sclerosis". Brain. 131 (7): 1759–1775. doi:10.1093/brain/awn098. PMC 2442427. PMID 18535080.
- Yiu EM, Laughlin S, Verhey LH, Banwell BL (2013). "Clinical and Magnetic Resonance Imaging (MRI) Distinctions Between Tumefactive Demyelination and Brain Tumors in Children". J Child Neurol. 29 (5): 654–65. doi:10.1177/0883073813500713. PMID 24092896.CS1 maint: multiple names: authors list (link)
- Mamilly, Ahmed; Aslan, Asala; Adeeb, Nimer; Al Asfari, Aya; Cuellar, Hugo (23 January 2020). "Tumefactive Multiple Sclerosis of the Cervical Spinal Cord: A Rare Case Report". Cureus. 12 (1): e6754. doi:10.7759/cureus.6754. PMC 7039350. PMID 32140322.
- Tintore M., Rovira A., Martinex M. J., Rio J., Diaz-Villoslada P., Brieva L.; et al. (2000). "Isolated demyelinating syndromes: comparison of different MR imaging criteria to predict conversion to clinically definite multiple sclerosis". AJNR Am J Neuroradiol. 21 (4): 702–706. PMID 10782781.CS1 maint: multiple names: authors list (link)
- Takeuchi T., Ogura M., Sato M., Kawai N., Tanihata H., Takasaka I., Minamiguchi H., Nakai M., Itakura T. (2008). "Late-onset tumefactive multiple sclerosis". Radiat Med. 26 (9): 549–552. doi:10.1007/s11604-008-0273-4. PMID 19030964.CS1 maint: multiple names: authors list (link)
- Sajja B. R., Wolinsky J. S., Narayana P. A. (2009). "Proton magnetic resonance spectroscopy in multiple sclerosis". Neuroimaging Clin N Am. 19 (1): 45–58. doi:10.1016/j.nic.2008.08.002. PMC 2615006. PMID 19064199.CS1 maint: multiple names: authors list (link)
- Ryotaro Ikeguchi et al., Proton magnetic resonance spectroscopy differentiates tumefactive demyelinating lesions from gliomas, Multiple Sclerosis and Related Disorders, August 2018, doi: https://doi.org/10.1016/j.msard.2018.08.025
- Kristen Krysko et al. Clinical Course, Radiologic Features and Treatment Response in Patients with Tumefactive Demyelinating Lesions in Toronto. Neurology 2015; vol. 84 no. 14 Supplement P4.018.
- Rocco; et al. (2016). "Tumefactive demyelinating lesions: spectrum of disease, diagnosis and treatment". Current Neurobiology.
- Shailee Shah, Sharon Stoll, Thomas Leist, Plasmapheresis in Corticosteroid-Resistant Acute Disseminated Demyelination: Report of Two Adult Cases, Neurology 2015; 84 no. 14 Supplement P4.048
- White LJ, Dressendorfer RH (2004). "Exercise and multiple sclerosis". Sports Med. 34 (15): 1077–100. doi:10.2165/00007256-200434150-00005. PMID 15575796.
- Lew K.; et al. (2016). "Role of Therapeutic Plasma Exchange in Treatment of Tumefactive Multiple Sclerosis-Associated Low CD4 and CD8 Levels". Case Rep Neurol. 8 (2): 179–184. doi:10.1159/000448704. PMC 5043263. PMID 27721782.
- Peterson JW, Trapp BD (2005). "Neuropathobiology of multiple sclerosis". Neurol Clin. 23 (1): 107–129. doi:10.1016/j.ncl.2004.09.008. PMID 15661090.
- National Multiple Sclerosis Society. "Epidemiology of MS". Retrieved 2012-11-17.
- Lattanzi S (2012). "Solitary sclerosis: Progressive myelopathy from solitary demyelinating lesion". Neurology. 79 (4): 393, author reply 393. doi:10.1212/01.wnl.0000418061.10382.f7. PMID 22826546.
- Ayrignac X, Carra-Dalliere C, Homeyer P, Labauge P (2013). "Solitary sclerosis: progressive myelopathy from solitary demyelinating lesion. A new entity?". Acta Neurol Belg. 113 (4): 533–4. doi:10.1007/s13760-013-0182-x. PMID 23358965.
- Schmalstieg William F., Keegan B. Mark, Weinshenker Brian G. (2012). "Progressive myelopathy from solitary demyelinating lesion". Neurology. 78 (8): 540–544. doi:10.1212/WNL.0b013e318247cc8c. PMID 22323754.CS1 maint: multiple names: authors list (link)
- Lattanzi Simona, Solitary (2012). "Progressive myelopathy from solitary demyelinating lesion". Neurology. 79 (4): 393. doi:10.1212/01.wnl.0000418061.10382.f7. PMID 22826546.
- Rathnasabapathi Devipriya, Elsone Liene, Krishnan Anita, Young Carolyn, Larner Andrew, Jacob Anu (2015). "Solitary sclerosis: Progressive neurological deficit from a spatially isolated demyelinating lesion: A further report". The Journal of Spinal Cord Medicine. 38 (4): 551–555. doi:10.1179/2045772314Y.0000000283. PMC 4612213. PMID 25615515.CS1 maint: multiple names: authors list (link)
- Christine Lebrun, Mikael Cohen, Lydiane Mondot, Xavier Ayrignac, Pierre Labauge, A Case Report of Solitary Sclerosis: This is Really Multiple Sclerosis. Neurology and Therapy, pp 1–5, 24 August 2017
- Tohyama, Sarasa et al, Trigeminal neuralgia associated with solitary pontine lesion, PAIN: December 09, 2019, doi: 10.1097/j.pain.0000000000001777
- Yaqing Shu Youming Long Shisi Wang Wanming Hu Jian Zhou Huiming Xu Chen Chen Yangmei Ou Zhengqi Lu Alexander Y. Lau Xinhua Yu Allan G. Kermode Wei Qiu, Brain histopathological study and prognosis in MOG antibody‐associated demyelinating pseudotumor, 08 January 2019, https://doi.org/10.1002/acn3.712