Hemodialysis
Hemodialysis, also spelled haemodialysis, or simply dialysis, is a process of purifying the blood of a person whose kidneys are not working normally. This type of dialysis achieves the extracorporeal removal of waste products such as creatinine and urea and free water from the blood when the kidneys are in a state of kidney failure. Hemodialysis is one of three renal replacement therapies (the other two being kidney transplant and peritoneal dialysis). An alternative method for extracorporeal separation of blood components such as plasma or cells is apheresis.
| Hemodialysis | |
|---|---|
 Hemodialysis machine | |
| Other names | kidney dialysis |
| Specialty | nephrology |
Hemodialysis can be an outpatient or inpatient therapy. Routine hemodialysis is conducted in a dialysis outpatient facility, either a purpose built room in a hospital or a dedicated, stand-alone clinic. Less frequently hemodialysis is done at home. Dialysis treatments in a clinic are initiated and managed by specialized staff made up of nurses and technicians; dialysis treatments at home can be self-initiated and managed or done jointly with the assistance of a trained helper who is usually a family member.[1]
Medical uses

Hemodialysis is the choice of renal replacement therapy for patients who need dialysis acutely, and for many patients as maintenance therapy. It provides excellent, rapid clearance of solutes.[2]
A nephrologist (a medical kidney specialist) decides when hemodialysis is needed and the various parameters for a dialysis treatment. These include frequency (how many treatments per week), length of each treatment, and the blood and dialysis solution flow rates, as well as the size of the dialyzer. The composition of the dialysis solution is also sometimes adjusted in terms of its sodium and potassium and bicarbonate levels. In general, the larger the body size of an individual, the more dialysis he/she will need. In North America and the UK, 3–4 hour treatments (sometimes up to 5 hours for larger patients) given 3 times a week are typical. Twice-a-week sessions are limited to patients who have a substantial residual kidney function. Four sessions per week are often prescribed for larger patients, as well as patients who have trouble with fluid overload. Finally, there is growing interest in short daily home hemodialysis, which is 1.5 – 4 hr sessions given 5–7 times per week, usually at home. There is also interest in nocturnal dialysis, which involves dialyzing a patient, usually at home, for 8–10 hours per night, 3–6 nights per week. Nocturnal in-center dialysis, 3–4 times per week, is also offered at a handful of dialysis units in the United States.
Adverse effects
Disadvantages
- Restricts independence, as people undergoing this procedure cannot travel around because of supplies' availability
- Requires more supplies such as high water quality and electricity
- Requires reliable technology like dialysis machines
- The procedure is complicated and requires that care givers have more knowledge
- Requires time to set up and clean dialysis machines, and expense with machines and associated staff[2]
Complications
Fluid shifts
Hemodialysis often involves fluid removal (through ultrafiltration), because most patients with renal failure pass little or no urine. Side effects caused by removing too much fluid and/or removing fluid too rapidly include low blood pressure, fatigue, chest pains, leg-cramps, nausea and headaches. These symptoms can occur during the treatment and can persist post treatment; they are sometimes collectively referred to as the dialysis hangover or dialysis washout. The severity of these symptoms is usually proportionate to the amount and speed of fluid removal. However, the impact of a given amount or rate of fluid removal can vary greatly from person to person and day to day. These side effects can be avoided and/or their severity lessened by limiting fluid intake between treatments or increasing the dose of dialysis e.g. dialyzing more often or longer per treatment than the standard three times a week, 3–4 hours per treatment schedule.
Access-related
Since hemodialysis requires access to the circulatory system, patients undergoing hemodialysis may expose their circulatory system to microbes, which can lead to bacteremia, an infection affecting the heart valves (endocarditis) or an infection affecting the bones (osteomyelitis). The risk of infection varies depending on the type of access used (see below). Bleeding may also occur, again the risk varies depending on the type of access used. Infections can be minimized by strictly adhering to infection control best practices.
Anticoagulation-related
Heparin is the most commonly used anticoagulant in hemodialysis, as it is generally well tolerated and can be quickly reversed with protamine sulfate. Heparin allergy can infrequently be a problem and can cause a low platelet count. In such patients, alternative anticoagulants can be used. In patients at high risk of bleeding, dialysis can be done without anticoagulation.
First-use syndrome
First-use syndrome is a rare but severe anaphylactic reaction to the artificial kidney. Its symptoms include sneezing, wheezing, shortness of breath, back pain, chest pain, or sudden death. It can be caused by residual sterilant in the artificial kidney or the material of the membrane itself. In recent years, the incidence of first-use syndrome has decreased, due to an increased use of gamma irradiation, steam sterilization, or electron-beam radiation instead of chemical sterilants, and the development of new semipermeable membranes of higher biocompatibility. New methods of processing previously acceptable components of dialysis must always be considered. For example, in 2008, a series of first-use type of reactions, including deaths, occurred due to heparin contaminated during the manufacturing process with oversulfated chondroitin sulfate.[3]
Cardiovascular
Longterm complications of hemodialysis include hemodialysis-associated amyloidosis, neuropathy and various forms of heart disease. Increasing the frequency and length of treatments has been shown to improve fluid overload and enlargement of the heart that is commonly seen in such patients.[4][5] Due to these complications, the prevalence of complementary and alternative medicine use is high among patients undergoing hemodialysis.[6][7]
Vitamin Deficiency
Folate deficiency can occur in some patients having hemodialysis.[8]
Mechanism and technique
.svg.png)
The principle of hemodialysis is the same as other methods of dialysis; it involves diffusion of solutes across a semipermeable membrane. Hemodialysis utilizes counter current flow, where the dialysate is flowing in the opposite direction to blood flow in the extracorporeal circuit. Counter-current flow maintains the concentration gradient across the membrane at a maximum and increases the efficiency of the dialysis.
Fluid removal (ultrafiltration) is achieved by altering the hydrostatic pressure of the dialysate compartment, causing free water and some dissolved solutes to move across the membrane along a created pressure gradient.
The dialysis solution that is used may be a sterilized solution of mineral ions. Urea and other waste products, potassium, and phosphate diffuse into the dialysis solution. However, concentrations of sodium and chloride are similar to those of normal plasma to prevent loss. Sodium bicarbonate is added in a higher concentration than plasma to correct blood acidity. A small amount of glucose is also commonly used.
Note that this is a different process to the related technique of hemofiltration.
Access
Three primary methods are used to gain access to the blood for hemodialysis: an intravenous catheter, an arteriovenous fistula (AV) and a synthetic graft. The type of access is influenced by factors such as the expected time course of a patient's renal failure and the condition of their vasculature. Patients may have multiple access procedures, usually because an AV fistula or graft is maturing and a catheter is still being used. The placement of a catheter is usually done under light sedation, while fistulas and grafts require an operation.

Types
There are three types of hemodialysis: conventional hemodialysis, daily hemodialysis, and nocturnal hemodialysis. Below is an adaptation and summary from a brochure of The Ottawa Hospital.
Conventional hemodialysis
Conventional hemodialysis is usually done three times per week, for about three to four hours for each treatment (Sometimes five hours for larger patients), during which the patient's blood is drawn out through a tube at a rate of 200–400 mL/min. The tube is connected to a 15, 16, or 17 gauge needle inserted in the dialysis fistula or graft, or connected to one port of a dialysis catheter. The blood is then pumped through the dialyzer, and then the processed blood is pumped back into the patient's bloodstream through another tube (connected to a second needle or port). During the procedure, the patient's blood pressure is closely monitored, and if it becomes low, or the patient develops any other signs of low blood volume such as nausea, the dialysis attendant can administer extra fluid through the machine. During the treatment, the patient's entire blood volume (about 5000 cc) circulates through the machine every 15 minutes. During this process, the dialysis patient is exposed to a week's worth of water for the average person.
Daily hemodialysis
Daily hemodialysis is typically used by those patients who do their own dialysis at home. It is less stressful (more gentle) but does require more frequent access. This is simple with catheters, but more problematic with fistulas or grafts. The "buttonhole technique" can be used for fistulas requiring frequent access. Daily hemodialysis is usually done for 2 hours six days a week.
Nocturnal hemodialysis
The procedure of nocturnal hemodialysis is similar to conventional hemodialysis except it is performed three to six nights a week and between six and ten hours per session while the patient sleeps.[9]
Equipment
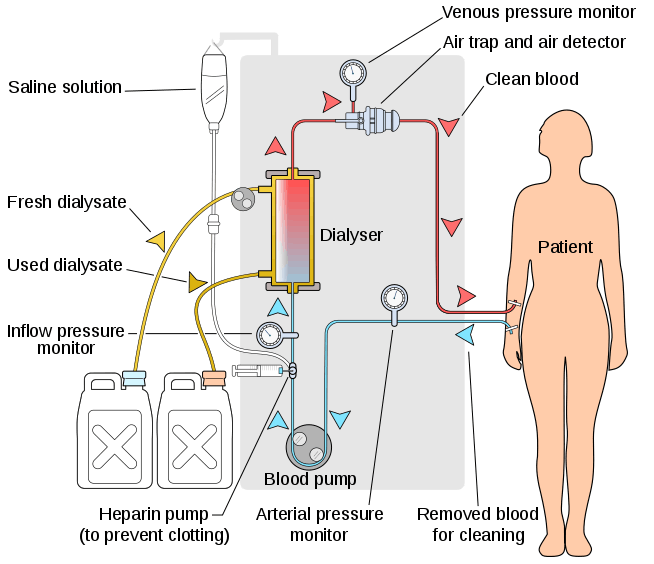
The hemodialysis machine pumps the patient's blood and the dialysate through the dialyzer. The newest dialysis machines on the market are highly computerized and continuously monitor an array of safety-critical parameters, including blood and dialysate flow rates; dialysis solution conductivity, temperature, and pH; and analysis of the dialysate for evidence of blood leakage or presence of air. Any reading that is out of normal range triggers an audible alarm to alert the patient-care technician who is monitoring the patient. Manufacturers of dialysis machines include companies such as Nipro, Fresenius, Gambro, Baxter, B. Braun, NxStage and Bellco.
Types
Water system

An extensive water purification system is absolutely critical for hemodialysis. Since dialysis patients are exposed to vast quantities of water, which is mixed with dialysate concentrate to form the dialysate, even trace mineral contaminants or bacterial endotoxins can filter into the patient's blood. Because the damaged kidneys cannot perform their intended function of removing impurities, ions introduced into the bloodstream via water can build up to hazardous levels, causing numerous symptoms or death. Aluminum, chloramine, fluoride, copper, and zinc, as well as bacterial fragments and endotoxins, have all caused problems in this regard.
For this reason, water used in hemodialysis is carefully purified before use. Initially it is filtered and temperature-adjusted and its pH is corrected by adding an acid or base. Then it is softened. Next the water is run through a tank containing activated charcoal to adsorb organic contaminants. Primary purification is then done by forcing water through a membrane with very tiny pores, a so-called reverse osmosis membrane. This lets the water pass, but holds back even very small solutes such as electrolytes. Final removal of leftover electrolytes is done by passing the water through a tank with ion-exchange resins, which remove any leftover anions or cations and replace them with hydroxyl and hydrogen ions, respectively, leaving ultrapure water.
Even this degree of water purification may be insufficient. The trend lately is to pass this final purified water (after mixing with dialysate concentrate) through a dialyzer membrane. This provides another layer of protection by removing impurities, especially those of bacterial origin, that may have accumulated in the water after its passage through the original water purification system.
Once purified water is mixed with dialysate concentrate, its conductivity increases, since water that contains charged ions conducts electricity. During dialysis, the conductivity of dialysis solution is continuously monitored to ensure that the water and dialysate concentrate are being mixed in the proper proportions. Both excessively concentrated dialysis solution and excessively dilute solution can cause severe clinical problems.
Dialyzer
The dialyzer is the piece of equipment that actually filters the blood. Almost all dialyzers in use today are of the hollow-fiber variety. A cylindrical bundle of hollow fibers, whose walls are composed of semi-permeable membrane, is anchored at each end into potting compound (a sort of glue). This assembly is then put into a clear plastic cylindrical shell with four openings. One opening or blood port at each end of the cylinder communicates with each end of the bundle of hollow fibers. This forms the "blood compartment" of the dialyzer. Two other ports are cut into the side of the cylinder. These communicate with the space around the hollow fibers, the "dialysate compartment." Blood is pumped via the blood ports through this bundle of very thin capillary-like tubes, and the dialysate is pumped through the space surrounding the fibers. Pressure gradients are applied when necessary to move fluid from the blood to the dialysate compartment.
Membrane and flux
Dialyzer membranes come with different pore sizes. Those with smaller pore size are called "low-flux" and those with larger pore sizes are called "high-flux." Some larger molecules, such as beta-2-microglobulin, are not removed at all with low-flux dialyzers; lately, the trend has been to use high-flux dialyzers. However, such dialyzers require newer dialysis machines and high-quality dialysis solution to control the rate of fluid removal properly and to prevent backflow of dialysis solution impurities into the patient through the membrane.
Dialyzer membranes used to be made primarily of cellulose (derived from cotton linter). The surface of such membranes was not very biocompatible, because exposed hydroxyl groups would activate complement in the blood passing by the membrane. Therefore, the basic, "unsubstituted" cellulose membrane was modified. One change was to cover these hydroxyl groups with acetate groups (cellulose acetate); another was to mix in some compounds that would inhibit complement activation at the membrane surface (modified cellulose). The original "unsubstituted cellulose" membranes are no longer in wide use, whereas cellulose acetate and modified cellulose dialyzers are still used. Cellulosic membranes can be made in either low-flux or high-flux configuration, depending on their pore size.
Another group of membranes is made from synthetic materials, using polymers such as polyarylethersulfone, polyamide, polyvinylpyrrolidone, polycarbonate, and polyacrylonitrile. These synthetic membranes activate complement to a lesser degree than unsubstituted cellulose membranes. Synthetic membranes can be made in either low- or high-flux configuration, but most are high-flux.
Nanotechnology is being used in some of the most recent high-flux membranes to create a uniform pore size. The goal of high-flux membranes is to pass relatively large molecules such as beta-2-microglobulin (MW 11,600 daltons), but not to pass albumin (MW ~66,400 daltons). Every membrane has pores in a range of sizes. As pore size increases, some high-flux dialyzers begin to let albumin pass out of the blood into the dialysate. This is thought to be undesirable, although one school of thought holds that removing some albumin may be beneficial in terms of removing protein-bound uremic toxins.
Membrane flux and outcome
Whether using a high-flux dialyzer improves patient outcomes is somewhat controversial, but several important studies have suggested that it has clinical benefits. The NIH-funded HEMO trial compared survival and hospitalizations in patients randomized to dialysis with either low-flux or high-flux membranes. Although the primary outcome (all-cause mortality) did not reach statistical significance in the group randomized to use high-flux membranes, several secondary outcomes were better in the high-flux group.[10][11] A recent Cochrane analysis concluded that benefit of membrane choice on outcomes has not yet been demonstrated.[12] A collaborative randomized trial from Europe, the MPO (Membrane Permeabilities Outcomes) study,[13] comparing mortality in patients just starting dialysis using either high-flux or low-flux membranes, found a nonsignificant trend to improved survival in those using high-flux membranes, and a survival benefit in patients with lower serum albumin levels or in diabetics.
Membrane flux and beta-2-microglobulin amyloidosis
High-flux dialysis membranes and/or intermittent on-line hemodiafiltration (IHDF) may also be beneficial in reducing complications of beta-2-microglobulin accumulation. Because beta-2-microglobulin is a large molecule, with a molecular weight of about 11,600 daltons, it does not pass at all through low-flux dialysis membranes. Beta-2-M is removed with high-flux dialysis, but is removed even more efficiently with IHDF. After several years (usually at least 5–7), patients on hemodialysis begin to develop complications from beta-2-M accumulation, including carpal tunnel syndrome, bone cysts, and deposits of this amyloid in joints and other tissues. Beta-2-M amyloidosis can cause very serious complications, including spondyloarthropathy, and often is associated with shoulder joint problems. Observational studies from Europe and Japan have suggested that using high-flux membranes in dialysis mode, or IHDF, reduces beta-2-M complications in comparison to regular dialysis using a low-flux membrane.[14][15][16][17][18]
Dialyzer size and efficiency
Dialyzers come in many different sizes. A larger dialyzer with a larger membrane area (A) will usually remove more solutes than a smaller dialyzer, especially at high blood flow rates. This also depends on the membrane permeability coefficient K0 for the solute in question. So dialyzer efficiency is usually expressed as the K0A – the product of permeability coefficient and area. Most dialyzers have membrane surface areas of 0.8 to 2.2 square meters, and values of K0A ranging from about 500 to 1500 mL/min. K0A, expressed in mL/min, can be thought of as the maximum clearance of a dialyzer at very high blood and dialysate flow rates.
Reuse of dialyzers
The dialyzer may either be discarded after each treatment or be reused. Reuse requires an extensive procedure of high-level disinfection. Reused dialyzers are not shared between patients. There was an initial controversy about whether reusing dialyzers worsened patient outcomes. The consensus today is that reuse of dialyzers, if done carefully and properly, produces similar outcomes to single use of dialyzers.[19]
Dialyzer Reuse is a practice that has been around since the invention of the product. This practice includes the cleaning of a used dialyzer to be reused multiple times for the same patient. Dialysis clinics reuse dialyzers to become more economical and reduce the high costs of “single-use” dialysis which can be extremely expensive and wasteful. Single used dialyzers are initiated just once and then thrown out creating a large amount of bio-medical waste with no mercy for cost savings. If done right, dialyzer reuse can be very safe for dialysis patients.
There are two ways of reusing dialyzers, manual and automated. Manual reuse involves the cleaning of a dialyzer by hand. The dialyzer is semi-disassembled then flushed repeatedly before being rinsed with water. It is then stored with a liquid disinfectant(PAA) for 18+ hours until its next use. Although many clinics outside the USA use this method, some clinics are switching toward a more automated/streamlined process as the dialysis practice advances. The newer method of automated reuse is achieved by means of a medical device which began in the early 1980s. These devices are beneficial to dialysis clinics that practice reuse – especially for large dialysis clinical entities – because they allow for several back to back cycles per day. The dialyzer is first pre-cleaned by a technician, then automatically cleaned by machine through a step-cycles process until it is eventually filled with liquid disinfectant for storage. Although automated reuse is more effective than manual reuse, newer technology has sparked even more advancement in the process of reuse. When reused over 15 times with current methodology, the dialyzer can lose B2m, middle molecule clearance and fiber pore structure integrity, which has the potential to reduce the effectiveness of the patient's dialysis session. Currently, as of 2010, newer, more advanced reprocessing technology has proven the ability to completely eliminate the manual pre-cleaning process altogether and has also proven the potential to regenerate (fully restore) all functions of a dialyzer to levels that are approximately equivalent to single-use for more than 40 cycles.[20] As medical reimbursement rates begin to fall even more, many dialysis clinics are continuing to operate effectively with reuse programs especially since the process is easier and more streamlined than before.
Epidemiology
Hemodialysis was one of the most common procedures performed in U.S. hospitals in 2011, occurring in 909,000 stays (a rate of 29 stays per 10,000 population). This was an increase of 68 percent from 1997, when there were 473,000 stays. It was the fifth most common procedure for patients aged 45–64 years.[21]
History
Many have played a role in developing dialysis as a practical treatment for renal failure, starting with Thomas Graham of Glasgow, who first presented the principles of solute transport across a semipermeable membrane in 1854.[22] The artificial kidney was first developed by Abel, Rountree, and Turner in 1913,[23] the first hemodialysis in a human being was by Hass (February 28, 1924)[24] and the artificial kidney was developed into a clinically useful apparatus by Kolff in 1943 – 1945.[25] This research showed that life could be prolonged in patients dying of kidney failure.
Willem Kolff was the first to construct a working dialyzer in 1943. The first successfully treated patient was a 67-year-old woman in uremic coma who regained consciousness after 11 hours of hemodialysis with Kolff's dialyzer in 1945. At the time of its creation, Kolff's goal was to provide life support during recovery from acute renal failure. After World War II ended, Kolff donated the five dialyzers he had made to hospitals around the world, including Mount Sinai Hospital, New York. Kolff gave a set of blueprints for his hemodialysis machine to George Thorn at the Peter Bent Brigham Hospital in Boston. This led to the manufacture of the next generation of Kolff's dialyzer, a stainless steel Kolff-Brigham dialysis machine.
According to McKellar (1999), a significant contribution to renal therapies was made by Canadian surgeon Gordon Murray with the assistance of two doctors, an undergraduate chemistry student, and research staff. Murray's work was conducted simultaneously and independently from that of Kolff. Murray's work led to the first successful artificial kidney built in North America in 1945–46, which was successfully used to treat a 26-year-old woman out of a uraemic coma in Toronto. The less-crude, more compact, second-generation "Murray-Roschlau" dialyser was invented in 1952–53, whose designs were stolen by German immigrant Erwin Halstrup, and passed off as his own (the "Halstrup–Baumann artificial kidney").[26]
By the 1950s, Willem Kolff's invention of the dialyzer was used for acute renal failure, but it was not seen as a viable treatment for patients with stage 5 chronic kidney disease (CKD). At the time, doctors believed it was impossible for patients to have dialysis indefinitely for two reasons. First, they thought no man-made device could replace the function of kidneys over the long term. In addition, a patient undergoing dialysis suffered from damaged veins and arteries, so that after several treatments, it became difficult to find a vessel to access the patient's blood.
The original Kolff kidney was not very useful clinically, because it did not allow for removal of excess fluid. Swedish professor Nils Alwall[27] encased a modified version of this kidney inside a stainless steel canister, to which a negative pressure could be applied, in this way effecting the first truly practical application of hemodialysis, which was done in 1946 at the University of Lund. Alwall also was arguably the inventor of the arteriovenous shunt for dialysis. He reported this first in 1948 where he used such an arteriovenous shunt in rabbits. Subsequently, he used such shunts, made of glass, as well as his canister-enclosed dialyzer, to treat 1500 patients in renal failure between 1946 and 1960, as reported to the First International Congress of Nephrology held in Evian in September 1960. Alwall was appointed to a newly created Chair of Nephrology at the University of Lund in 1957. Subsequently, he collaborated with Swedish businessman Holger Crafoord to found one of the key companies that would manufacture dialysis equipment in the past 50 years, Gambro. The early history of dialysis has been reviewed by Stanley Shaldon.[28]
Belding H. Scribner, working with the biomechanical engineer Wayne Quinton, modified the glass shunts used by Alwall by making them from Teflon. Another key improvement was to connect them to a short piece of silicone elastomer tubing. This formed the basis of the so-called Scribner shunt, perhaps more properly called the Quinton-Scribner shunt. After treatment, the circulatory access would be kept open by connecting the two tubes outside the body using a small U-shaped Teflon tube, which would shunt the blood from the tube in the artery back to the tube in the vein.[29]
In 1962, Scribner started the world's first outpatient dialysis facility, the Seattle Artificial Kidney Center, later renamed the Northwest Kidney Centers. Immediately the problem arose of who should be given dialysis, since demand far exceeded the capacity of the six dialysis machines at the center. Scribner decided that he would not make the decision about who would receive dialysis and who would not. Instead, the choices would be made by an anonymous committee, which could be viewed as one of the first bioethics committees.
For a detailed history of successful and unsuccessful attempts at dialysis, including pioneers such as Abel and Roundtree, Haas, and Necheles, see this review by Kjellstrand.[30]
References
- National Kidney and Urologic Diseases Information Clearinghouse guidance Kidney Failure: Choosing a Treatment That's Right for You Archived 2010-09-16 at the Wayback Machine
- Daugirdas J. T., Black P.G., Ing T.S. In "Handbook of Dialysis". 4th ed. Philadelphia, PA:Lippincott Williams & Wilkins, a Wolters Kluwer Business; 2007.
- Kishimoto TK, Viswanathan K, Ganguly T, et al. (2008). "Contaminated heparin associated with adverse clinical events and activation of the contact system". N Engl J Med. 358 (23): 2457–67. doi:10.1056/NEJMoa0803200. PMC 3778681. PMID 18434646.
- Ayus JC, Mizani MR, Achinger SG, Thadhani R, Go AS, Lee S (September 2005). "Effects of short daily versus conventional hemodialysis on left ventricular hypertrophy and inflammatory markers: a prospective, controlled study". Journal of the American Society of Nephrology. 16 (9): 2778–88. doi:10.1681/ASN.2005040392. PMID 16033855.
- Weinreich T, De los Ríos T, Gauly A, Passlick-Deetjen J (2006). "Effects of an increase in time vs. frequency on cardiovascular parameters in chronic hemodialysis patients". Clin. Nephrol. 66 (6): 433–9. doi:10.5414/CNP66433. PMID 17176915.
- Heydari M, Hashempur MH, Zargaran A (2013). "Use of herbal remedies among patients undergoing hemodialysis". Iran J Kidney Dis. 11 (1): 101–12. PMID 23883087.
- Birdee GS, Phillips RS, Brown RS (2013). "Use of Complementary and Alternative Medicine among Patients with End-Stage Renal Disease". Evidence-Based Complementary and Alternative Medicine. 2013: 1–6. doi:10.1155/2013/654109. PMC 3655568. PMID 23710227.
- Vitamin Deficiency Anemia, Mayo Clinic
- The Ottawa Hospital (TOH). Guide: Treatment options for chronic kidney disease. Ottawa, Ontario:The Ottawa Hospital Riverside Campus;2008
- Eknoyan G, Beck GJ, Cheung AK, et al. (2002). "Effect of dialysis dose and membrane flux in maintenance hemodialysis". N. Engl. J. Med. 347 (25): 2010–9. doi:10.1056/NEJMoa021583. PMID 12490682.
- Cheung AK, Levin NW, Greene T, et al. (2003). "Effects of high-flux hemodialysis on clinical outcomes: results of the HEMO study". J. Am. Soc. Nephrol. 14 (12): 3251–63. doi:10.1097/01.ASN.0000096373.13406.94. PMID 14638924.
- Macleod AM, Campbell M, Cody JD, et al. (2005). MacLeod AM (ed.). "Cellulose, modified cellulose and synthetic membranes in the haemodialysis of patients with end-stage renal disease". Cochrane Database Syst Rev (3): CD003234. doi:10.1002/14651858.CD003234.pub2. PMID 16034894.
- Locatelli F, Martin-Malo A, Hannedouche T, et al. (2009). "Effect of Membrane Permeability on Survival of Hemodialysis Patients". J Am Soc Nephrol. 20 (3): 645–54. doi:10.1681/ASN.2008060590. PMC 2653681. PMID 19092122.
- van Ypersele de Strihou C, Jadoul M, Malghem J, Maldague B, Jamart J (1991). "Effect of dialysis membrane and patient's age on signs of dialysis-related amyloidosis. The Working Party on Dialysis Amyloidosis". Kidney Int. 39 (5): 1012–9. doi:10.1038/ki.1991.128. PMID 2067196.
- KDOQI Clinical Practice Guidelines for Hemodialysis Adequacy, 2006 Updates. CPR 5. Archived 2007-06-30 at the Wayback Machine
- Küchle C, Fricke H, Held E, Schiffl H (1996). "High-flux hemodialysis postpones clinical manifestation of dialysis-related amyloidosis". Am. J. Nephrol. 16 (6): 484–8. doi:10.1159/000169048. PMID 8955759.
- Koda Y, Nishi S, Miyazaki S, et al. (1997). "Switch from conventional to high-flux membrane reduces the risk of carpal tunnel syndrome and mortality of hemodialysis patients". Kidney Int. 52 (4): 1096–101. doi:10.1038/ki.1997.434. PMID 9328951.
- Locatelli F, Mastrangelo F, Redaelli B, et al. (1996). "Effects of different membranes and dialysis technologies on patient treatment tolerance and nutritional parameters. The Italian Cooperative Dialysis Study Group". Kidney Int. 50 (4): 1293–302. doi:10.1038/ki.1996.441. PMID 8887291.
- KDOQI Clinical Practice Guidelines for Hemodialysis Adequacy, 2006 Updates Archived 2007-06-30 at the Wayback Machine. CPR 5.
- Strain, Nick. "Dialysis Tech". Dialysis Clinic.
- Pfuntner A., Wier L.M., Stocks C. Most Frequent Procedures Performed in U.S. Hospitals, 2011. HCUP Statistical Brief #165. October 2013. Agency for Healthcare Research and Quality, Rockville, MD. .
- Graham T. The Bakerian lecture: on osmotic force. Philosophical Transactions of the Royal Society in London. 1854;144:177–228.
- Abel, J. J., Rountree, L. G., and Turner, B. B. The removal of diffusible substances from the circulating blood by means of dialysis. Tn. Assoc. Am. Phys., 28:51, 1913.
- Georg Haas (1886–1971): The Forgotten Hemodialysis Pioneer (PDF) Archived 2007-12-02 at the Wayback Machine
- Kolff, W. J., and Berk, H. T. J. Artificial kidney, dialyzer with great area. Geneesk. gids., 21:1944.
- McKellar, S (1999). "Gordon Murray and the artificial kidney in Canada". Nephrology, Dialysis, Transplantation. 14 (11): 2766–70. doi:10.1093/ndt/14.11.2766. PMID 10534530.
- University of Lund website: Nils Alwall. Archived 2007-10-01 at the Wayback Machine
- Shaldon S. Development of Hemodialysis, From Access to Machine (presentation given during a symposium entitled: Excellence in Dialysis: Update in Nephrology; Karachi, Pakistan. October, 2002, as archived on HDCN
- "NIDDK Contributions to Dialysis". Archived from the original on 2009-01-13. Retrieved 2007-10-09.
- Kjellstrand CM. History of Dialysis, Men and Ideas. Talk given to the Nordic Nephrology Days Symposium, Lund, 1997, as archived on HDCN.
External links
| Wikimedia Commons has media related to Hemodialysis. |
- Your Kidneys and How They Work – (American) National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), NIH.
- Treatment Methods for Kidney Failure – (American) National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), NIH.
- Treatment Methods for Kidney Failure: Hemodialysis – (American) National Kidney and Urologic Diseases Information Clearinghouse, NIH.
| Fields | |
|---|---|
| Concepts | |
| Treatments | |
| Incidents | |
| Related topics |
|
| |