Dialysis disequilibrium syndrome
Dialysis disequilibrium syndrome (DDS) is the collection of neurological signs and symptoms, attributed to cerebral edema, during or following shortly after intermittent hemodialysis[1] or CRRT.[2]
| Dialysis disequilibrium syndrome | |
|---|---|
 | |
| Specialty | Neurology, nephrology |
Classically, DDS arises in individuals starting hemodialysis due to end-stage chronic kidney disease and is associated, in particular, with "aggressive" (high solute removal) dialysis.[3] However, it may also arise in fast onset, i.e. acute kidney failure in certain conditions.
Causes
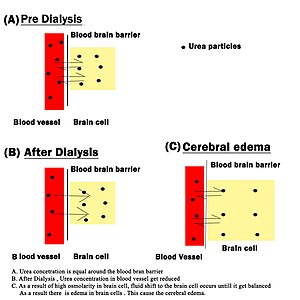
The cause of DDS is currently not well understood. There are two theories to explain it; the first theory postulates that urea transport from the brain cells is slowed in chronic kidney disease, leading to a large urea concentration gradient, which results in reverse osmosis. The second theory postulates that organic compounds are increased in uremia to protect the brain and result in injury by, like in the first theory, reverse osmosis.[1] More recent studies on rats noted that brain concentrations of organic osmolytes were not increased relative to baseline after rapid dialysis. Cerebral edema was thus attributed to osmotic effects related to a high urea gradient between plasma and brain.[4]
Symptoms
Symptoms of the mild degree of Disequilibrium syndrome is often missed with other dialysis complications. Like malignant hypertension, uremia, encephalopathy, subdural haemorrage, hyper and hypoglycaemia, electrolyte imbalances etc. However moderate and severe degree of DDS should not be missed and need immediate care. Unless it would result in severe neurological issues and finally death.
1. Headache
2. Nausea
3. Dizziness
4. Confusion
5. Visual disturbance
6. Tremor
7. Seizures
8. Coma
Diagnosis
Clinical signs of cerebral edema, such as focal neurological deficits, papilledema[5] and decreased level of consciousness, if temporally associated with recent hemodialysis, suggest the diagnosis. A computed tomography of the head is typically done to rule-out other intracranial causes.
MRI of the head has been used in research to better understand DDS.[6]
Treatment
Avoidance is the primary treatment. Better alternatives are Nocturnal or Daily Dialysis, which are far more gentle processes for the new dialysis patient. Dialysis disequilibrium syndrome is a reason why hemodialysis initiation should be done gradually, i.e. it is a reason why the first few dialysis sessions are shorter and less aggressive than the typical dialysis treatment for end-stage renal disease patients.
See also
References
- Bagshaw SM, Peets AD, Hameed M, Boiteau PJ, Laupland KB, Doig CJ (2004). "Dialysis Disequilibrium Syndrome: Brain death following hemodialysis for metabolic acidosis and acute renal failure – A case report". BMC Nephrol. 5: 9. doi:10.1186/1471-2369-5-9. PMC 515303. PMID 15318947. Free Full Text
- Mistry K. (2019). Dialysis disequilibrium syndrome prevention and management. International journal of nephrology and renovascular disease, 12, 69–77. https://doi.org/10.2147/IJNRD.S165925
- Port FK, Johnson WJ, Klass DW (1973). "Prevention of dialysis disequilibrium syndrome by use of high sodium concentration in the dialysate". Kidney Int. 3 (5): 327–33. doi:10.1038/ki.1973.51. PMID 4792047. Free Full Text.
- Silver, S. M. (December 1995). "Cerebral edema after rapid dialysis is not caused by an increase in brain organic osmolytes". Journal of the American Society of Nephrology. 6 (6): 1600–1606. PMID 8749686.
- Im L, Atabay C, Eller AW (2007). "Papilledema associated with dialysis disequilibrium syndrome". Semin Ophthalmol. 22 (3): 133–5. doi:10.1080/08820530701421585. PMID 17763231.
- Chen CL, Lai PH, Chou KJ, Lee PT, Chung HM, Fang HC (2007). "A preliminary report of brain edema in patients with uremia at first hemodialysis: evaluation by diffusion-weighted MR imaging". AJNR Am J Neuroradiol. 28 (1): 68–71. PMID 17213426.