Case–control study
A case–control study (also known as case–referent study) is a type of observational study in which two existing groups differing in outcome are identified and compared on the basis of some supposed causal attribute. Case–control studies are often used to identify factors that may contribute to a medical condition by comparing subjects who have that condition/disease (the "cases") with patients who do not have the condition/disease but are otherwise similar (the "controls").[1] They require fewer resources but provide less evidence for causal inference than a randomized controlled trial. A case–control study produces only an odds ratio, which is an inferior measure of strength of association compared to relative risk.
Definition
The case–control is a type of epidemiological observational study. An observational study is a study in which subjects are not randomized to the exposed or unexposed groups, rather the subjects are observed in order to determine both their exposure and their outcome status and the exposure status is thus not determined by the researcher.
Porta's Dictionary of Epidemiology defines the case–control study as: an observational epidemiological study of persons with the disease (or another outcome variable) of interest and a suitable control group of persons without the disease (comparison group, reference group).[2] The potential relationship of a suspected risk factor or an attribute to the disease is examined by comparing the diseased and nondiseased subjects with regard to how frequently the factor or attribute is present (or, if quantitative, the levels of the attribute) in each of the groups (diseased and nondiseased)."[2]
For example, in a study trying to show that people who smoke (the attribute) are more likely to be diagnosed with lung cancer (the outcome), the cases would be persons with lung cancer, the controls would be persons without lung cancer (not necessarily healthy), and some of each group would be smokers. If a larger proportion of the cases smoke than the controls, that suggests, but does not conclusively show, that the hypothesis is valid.
The case–control study is frequently contrasted with cohort studies, wherein exposed and unexposed subjects are observed until they develop an outcome of interest.[2][3]
Control group selection
Controls need not be in good health; inclusion of sick people is sometimes appropriate, as the control group should represent those at risk of becoming a case.[4] Controls should come from the same population as the cases, and their selection should be independent of the exposures of interest.[5]
Controls can carry the same disease as the experimental group, but of another grade/severity, therefore being different from the outcome of interest. However, because the difference between the cases and the controls will be smaller, this results in a lower power to detect an exposure effect.
As with any epidemiological study, greater numbers in the study will increase the power of the study. Numbers of cases and controls do not have to be equal. In many situations, it is much easier to recruit controls than to find cases. Increasing the number of controls above the number of cases, up to a ratio of about 4 to 1, may be a cost-effective way to improve the study.[4]
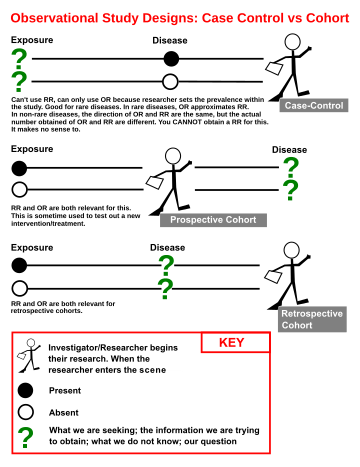
Prospective vs. retrospective cohort studies[6]
A prospective study watches for outcomes, such as the development of a disease, during the study period and relates this to other factors such as suspected risk or protection factor(s). The study usually involves taking a cohort of subjects and watching them over a long period. The outcome of interest should be common; otherwise, the number of outcomes observed will be too small to be statistically meaningful (indistinguishable from those that may have arisen by chance). All efforts should be made to avoid sources of bias such as the loss of individuals to follow up during the study. Prospective studies usually have fewer potential sources of bias and confounding than retrospective studies.
A retrospective study, on the other hand, looks backwards and examines exposures to suspected risk or protection factors in relation to an outcome that is established at the start of the study. Many valuable case-control studies, such as Lane and Claypon's 1926 investigation of risk factors for breast cancer, were retrospective investigations. Most sources of error due to confounding and bias are more common in retrospective studies than in prospective studies. For this reason, retrospective investigations are often criticised. If the outcome of interest is uncommon, however, the size of prospective investigation required to estimate relative risk is often too large to be feasible. In retrospective studies the odds ratio provides an estimate of relative risk. One should take special care to avoid sources of bias and confounding in retrospective studies.
Strengths and weaknesses
Case–control studies are a relatively inexpensive and frequently used type of epidemiological study that can be carried out by small teams or individual researchers in single facilities in a way that more structured experimental studies often cannot be. They have pointed the way to a number of important discoveries and advances. The case–control study design is often used in the study of rare diseases or as a preliminary study where little is known about the association between the risk factor and disease of interest.[7]
Compared to prospective cohort studies they tend to be less costly and shorter in duration. In several situations, they have greater statistical power than cohort studies, which must often wait for a 'sufficient' number of disease events to accrue.
Case–control studies are observational in nature and thus do not provide the same level of evidence as randomized controlled trials. The results may be confounded by other factors, to the extent of giving the opposite answer to better studies. A meta-analysis of what was considered 30 high-quality studies concluded that use of a product halved a risk, when in fact the risk was, if anything, increased.[8][9] It may also be more difficult to establish the timeline of exposure to disease outcome in the setting of a case–control study than within a prospective cohort study design where the exposure is ascertained prior to following the subjects over time in order to ascertain their outcome status. The most important drawback in case–control studies relates to the difficulty of obtaining reliable information about an individual's exposure status over time. Case–control studies are therefore placed low in the hierarchy of evidence.
Examples
One of the most significant triumphs of the case–control study was the demonstration of the link between tobacco smoking and lung cancer, by Richard Doll and Bradford Hill. They showed a statistically significant association in a large case–control study.[10] Opponents argued for many years that this type of study cannot prove causation, but the eventual results of cohort studies confirmed the causal link which the case–control studies suggested,[11][12] and it is now accepted that tobacco smoking is the cause of about 87% of all lung cancer mortality in the US.
Analysis
Case–control studies were initially analyzed by testing whether or not there were significant differences between the proportion of exposed subjects among cases and controls.[13] Subsequently, Cornfield[14] pointed out that, when the disease outcome of interest is rare, the odds ratio of exposure can be used to estimate the relative risk (see rare disease assumption). The validity of the odds ratio depends highly on the nature of the disease studied, on the sampling methodology and on the type of follow-up. Although in classical case-control studies, it remains true that the odds ratio can only approximate the relative risk in the case of rare diseases, there is a number of other types of studies (case-cohort, nested case-control, cohort studies) in which it was later shown that the odds ratio of exposure can be used to estimate the relative risk or the incidence rate ratio of exposure without the need for the rare disease assumption.[13][15][16]
When the logistic regression model is used to model the case-control data and the odds ratio is of interest, both the prospective and retrospective likelihood methods will lead to identical maximum likelihood estimations for covariate, except for the intercept. [17]
References
- "8. Case–control and cross sectional studies" (PDF). Retrieved 5 March 2012.
- Porta, M., ed. (2008). A Dictionary of Epidemiology (5th ed.). New York: Oxford University Press. ISBN 978-0-19-531450-2.
- Rothman, K. (2002). Epidemiology: An Introduction. Oxford, England: Oxford University Press. ISBN 978-0-19-513554-1.
- Grimes DA, Schulz KF (2005). "Compared to what? Finding controls for case–control studies". Lancet. 365 (9468): 1429–33. doi:10.1016/S0140-6736(05)66379-9. PMID 15836892.CS1 maint: uses authors parameter (link)
- Schulz KF, Grimes DA (2002). "Case–control studies: research in reverse". Lancet. 359 (9304): 431–4. doi:10.1016/S0140-6736(02)07605-5. PMID 11844534.CS1 maint: uses authors parameter (link)
- "Prospective, Retrospective, Case-control, Cohort Studies - StatsDirect". www.statsdirect.com. Retrieved 4 July 2019.
- Levin KA (2005). "Study design I". Evidence-Based Dentistry. 6 (3): 78–79. doi:10.1038/sj.ebd.6400355. PMID 16184164.CS1 maint: uses authors parameter (link)
- Lawlor DA, Davey Smith G, Ebrahim S (2004). "Commentary: the hormone replacement-coronary heart disease conundrum: is this the death of observational epidemiology?". Int J Epidemiol. 33 (3): 464–7. doi:10.1093/ije/dyh124. PMID 15166201.CS1 maint: uses authors parameter (link)
- Ioannidis JP (2005). "Contradicted and initially stronger effects in highly cited clinical research". JAMA. 294 (2): 218–28. doi:10.1001/jama.294.2.218. PMID 16014596.CS1 maint: uses authors parameter (link)
- Doll R, Hill AB (1950). "Smoking and carcinoma of the lung; preliminary report". Br Med J. 2 (4682): 739–48. doi:10.1136/bmj.2.4682.739. PMC 2038856. PMID 14772469.CS1 maint: uses authors parameter (link)
- Doll R, Hill AB (1956). "Lung cancer and other causes of death in relation to smoking; a second report on the mortality of British doctors". Br Med J. 2 (5001): 1071–81. doi:10.1136/bmj.2.5001.1071. PMC 2035864. PMID 13364389.CS1 maint: uses authors parameter (link)
- Doll R, Peto R, Boreham J, Sutherland I (2004). "Mortality in relation to smoking: 50 years' observations on male British doctors". BMJ. 328 (7455): 1519. doi:10.1136/bmj.38142.554479.AE. PMC 437139. PMID 15213107.CS1 maint: uses authors parameter (link)
- Rodrigues, L.; Kirkwood, B. R. (1990). "Case–control designs in the study of common diseases: updates on the demise of the rare disease assumption and the choice of sampling scheme for controls". Int. J. Epidemiol. 19 (1): 205–13. doi:10.1093/ije/19.1.205. PMID 2190942.
- Greenhouse SW (1982). "Jerome Cornfield's contributions to epidemiology". Biometrics. 38 Suppl: 33–45. doi:10.2307/2529852. PMID 7046823.CS1 maint: uses authors parameter (link)
- Miettinen, O. (1976). "Estimability and estimation in case–referent studies". Am. J. Epidemiol. 103 (2): 226–35. doi:10.1093/oxfordjournals.aje.a112220. PMID 1251836.
- Rothman, K. J.; Greenland, S.; Lash, T. L. (2008). Modern Epidemiology (3rd ed.). Wolters Kluwer, Lippincott Williams & Wilkins. ISBN 978-0-7817-5564-1.
- Prentice RL, Pyke R (1979). "Logistic disease incidence models and case-control studies". Biometrika. 66: 403–411.
Further reading
- Stolley, Paul D.; Schlesselman, James J. (1982). Case–control studies: design, conduct, analysis. Oxford [Oxfordshire]: Oxford University Press. ISBN 0-19-502933-X. (Still a very useful book, and a great place to start, but now a bit out of date.)