Hypomania
Hypomania (literally "under mania" or "less than mania") is a mood state characterized by persistent disinhibition and mood elevation (euphoria), with behavior that is noticeably different from the person's typical behavior when in a non-depressed state. It may involve irritability, not necessarily less severe than full mania; in fact, the presence of marked irritability is a documented feature of hypomanic and mixed episodes in Bipolar type II. According to DSM-5 criteria, hypomania is distinct from mania in that there is no significant functional impairment; mania, by DSM-5 definition, does include significant functional impairment and may have psychotic features.
| Hypomania | |
|---|---|
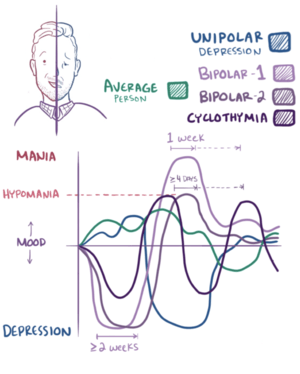 | |
| Graphical representation of hypomania and mania | |
| Specialty | Psychiatry, Clinical Psychology |
Characteristic behaviors of persons experiencing hypomania are a notable decrease in the need for sleep, an overall increase in energy, unusual behaviors and actions, and a markedly distinctive increase in talkativeness and confidence, commonly exhibited with a flight of creative ideas. Other symptoms related to this may include feelings of grandiosity, distractibility, and hypersexuality.[1] While hypomanic behavior often generates productivity and excitement, it can become troublesome if the subject engages in risky or otherwise inadvisable behaviors, and/or the symptoms manifest themselves in trouble with everyday life events.[2] When manic episodes are separated into stages of a progression according to symptomatic severity and associated features, hypomania constitutes the first stage of the syndrome, wherein the cardinal features (euphoria or heightened irritability, pressure of speech and activity, increased energy, decreased need for sleep, and flight of ideas) are most plainly evident.
Signs and symptoms
Individuals in a hypomanic state have a decreased need for sleep, are extremely gregarious and competitive, and have a great deal of energy. They are, otherwise, often fully functioning (unlike individuals suffering from a full manic episode).[3]
Distinctive markers
Specifically, hypomania is distinguished from mania by the absence of psychotic symptoms and grandiosity, and by its lesser degree of impact on functioning.[4][5]
Hypomania is a feature of bipolar II disorder and cyclothymia, but can also occur in schizoaffective disorder.[5] Hypomania is also a feature of bipolar I disorder; it arises in sequential procession as the mood disorder fluctuates between normal mood (euthymia) and mania. Some individuals with bipolar I disorder have hypomanic as well as manic episodes. Hypomania can also occur when moods progress downwards from a manic mood state to a normal mood. Hypomania is sometimes credited with increasing creativity and productive energy. Numerous people with bipolar disorder have credited hypomania with giving them an edge in their theater of work.[6][7]
People who experience hyperthymia, or "chronic hypomania",[8] encounter the same symptoms as hypomania but on a longer-term basis.[9]
Associated disorders
Cyclothymia, a condition of continuous mood fluctuations, is characterized by oscillating experiences of hypomania and depression that fail to meet the diagnostic criteria for either manic or major depressive episodes. These periods are often interspersed with periods of relatively normal (euthymic) functioning.[10]
When a patient presents with a history of at least one episode of both hypomania and major depression, each of which meet the diagnostic criteria, bipolar II disorder is diagnosed. In some cases, depressive episodes routinely occur during the fall or winter and hypomanic ones in the spring or summer. In such cases, one speaks of a "seasonal pattern".[11]
If left untreated, and in those so predisposed, hypomania may transition into mania, which may be psychotic, in which case bipolar I disorder is the correct diagnosis.[12]
Causes
Often in those who have experienced their first episode of hypomania – generally without psychotic features – there may be a long or recent history of depression or a mix of hypomania combined with depression (known as mixed-state) prior to the emergence of manic symptoms. This commonly surfaces in the mid to late teens. Because the teenage years are typically an emotionally charged time of life, it is not unusual for mood swings to be passed off as normal hormonal teen behavior and for a diagnosis of bipolar disorder to be missed until there is evidence of an obvious manic or hypomanic phase.[13]
In cases of drug-induced hypomanic episodes in unipolar depressives, the hypomania can almost invariably be eliminated by lowering medication dosage, withdrawing the drug entirely, or changing to a different medication if discontinuation of treatment is not possible.[14]
Hypomania can be associated with narcissistic personality disorder.[15]
Psychopathology
Mania and hypomania are usually studied together as components of bipolar disorders, and the pathophysiology is usually assumed to be the same. Given that norepinephrine and dopaminergic drugs are capable of triggering hypomania, theories relating to monoamine hyperactivity have been proposed. A theory unifying depression and mania in bipolar individuals proposes that decreased serotonergic regulation of other monoamines can result in either depressive or manic symptoms. Lesions on the right side frontal and temporal lobes have further been associated with mania.[16]
Diagnosis
The DSM-IV-TR defines a hypomanic episode as including, over the course of at least four days, elevated mood plus three of the following symptoms OR irritable mood plus four of the following symptoms, when the behaviors are clearly different from how the person typically acts when not depressed:
- pressured speech
- inflated self-esteem or grandiosity
- decreased need for sleep
- flight of ideas or the subjective experience that thoughts are racing
- easily distracted
- increase in goal-directed activity (e.g., social activity, at work, or hypersexuality), or psychomotor agitation
- involvement in pleasurable activities that may have a high potential for negative psycho-social or physical consequences (e.g., the person engages in unrestrained buying sprees, sexual indiscretions, reckless driving, physical and verbal conflicts, foolish business investments, quitting a job to pursue some grandiose goal, etc).[17]
Medications
Antimanic drugs are used to control acute attacks and prevent recurring episodes of hypomania combined with a range of psychological therapies.[18] The recommended length of treatment ranges from 2 years to 5 years. Anti-depressants may also be required for existing treatments but are avoided in patients who have had a recent history with hypomania.[19] Sertraline has often been debated to have side effects that can trigger hypomania.[20][21]
These include:[22]
Other anti-manic drugs that are not antipsychotics include:
Other drugs used to treat symptoms of mania/hypomania but considered less effective include:
Etymology
The Ancient Greek physician Hippocrates called one personality type 'hypomanic' (Greek: ὑπομαινόμενοι, hypomainómenoi).[23][24] In 19th century psychiatry, when mania had a broad meaning of insanity, hypomania was equated by some to concepts of 'partial insanity' or monomania.[25][26][27] A more specific usage was advanced by the German neuro-psychiatrist Emanuel Ernst Mendel in 1881, who wrote, "I recommend, taking into consideration the word used by Hippocrates, to name those types of mania that show a less severe phenomenological picture, 'hypomania'".[23][28] Narrower operational definitions of hypomania were developed in the 1960s and 1970s.
See also
- Bipolar disorder
- Bipolar I
- Bipolar II
- Borderline personality disorder
- Clinical depression
- Creativity and mental illness
- Cyclothymia
- Hyperthymic temperament
- Bertram D. Lewin
- Mania
- Narcissistic personality disorder
- People with bipolar disorder
- Regression (psychology)
- Schizoaffective disorder
References
- Mania and Hypomania Archived 2015-04-02 at the Wayback Machine
- Understanding Hypomania and Mania Archived 2015-03-27 at the Wayback Machine
- "Bipolar Disorder in Adults" (PDF). NIH Publication No. 12-3679. National Institute of Mental Health. 2012. Archived from the original (PDF) on 2015-05-01.
- Goodwin, Guy (2 January 2018). "Hypomania: What's in a name?". British Journal of Psychiatry. 181 (2): 94–95. doi:10.1192/bjp.181.2.94.
- British Psychological Society, National Collaborating Centre for Mental Health (Great Britain), National Institute for Health and Clinical Excellence (Great Britain) (2006). Bipolar Disorder: The Management of Bipolar Disorder in Adults, Children and Adolescents, in Primary and Secondary Care. Leicester; London: British Psychological Society; Royal College of Psychiatrists. ISBN 978-1-85433-441-1. Archived from the original on 9 May 2018. Retrieved 3 December 2015.
- Doran, Christopher (2008). The hypomania handbook : the challenge of elevated mood. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 16. ISBN 9780781775205. Retrieved 3 December 2015.
- Kaufman, James (2014). Creativity and mental illness. Cambridge: Cambridge University Press. p. 214. ISBN 9781316003626. Retrieved 3 December 2015.
- Ghaemi, S Nassir (2003). Mood disorders : a practical guide. Philadelphia: Lippincott Williams & Wilkins. p. 48. ISBN 9780781727839. Retrieved 4 December 2015.
- Bloch, Jon (2006). The everything health guide to adult bipolar disorder : reassuring advice to help you cope. Avon, Mass.: Adams Media. p. 12. ISBN 9781593375850. Retrieved 4 December 2015.
hyperthymia.
- "Cyclothymia". BehaveNet Clinical Capsules. Archived from the original on 2008-03-14. Retrieved 2008-01-03.
- "Bipolar II Disorder". BehaveNet Clinical Capsules. Archived from the original on 2008-03-14. Retrieved 2008-01-03.
- Post Robert M (2007). "Kindling and sensitization as models for affective episode recurrence, cyclicity, and tolerance phenomena". Neuroscience & Biobehavioral Reviews. 31 (6): 858–873. doi:10.1016/j.neubiorev.2007.04.003. PMID 17555817.
- Drug-Induced Dysfunction in Psychiatry. Matcheri S. Keshavan and John S. Kennedy, Editors (Taylor & Francis, 1992).
- Bipolar Disorder: A Summary of Clinical Issues and Treatment Options. Bipolar Disorder Sub-Committee, Canadian Network for Mood and Anxiety Treatments (CANMAT). April 1997
- Daniel Fulford; Sheri L. Johnson; Charles S. Carver (December 2008). "Commonalities and differences in characteristics of persons at risk for narcissism and mania". J Res Pers. 42 (6): 1427–1438. doi:10.1016/j.jrp.2008.06.002. PMC 2849176. PMID 20376289.
- Hilty, Donald M.; Leamon, Martin H.; Lim, Russell F.; Kelly, Rosemary H.; Hales, Robert E. (8 January 2017). "A Review of Bipolar Disorder in Adults". Psychiatry (Edgmont). 3 (9): 43–55. ISSN 1550-5952. PMC 2963467. PMID 20975827.
- "Hypomanic Episode". BehaveNet Clinical Capsules. Archived from the original on 2007-10-24. Retrieved 2008-01-03.
- "Hypomania and mania". NHS. Retrieved 2019-07-04.
- "Mania and hypomania". bnf. Retrieved 2019-07-03.
- Mendhekar, D. N.; Gupta, D.; Girotra, V. (13 June 2003). "Sertraline‐induced hypomania: a genuine side‐effect". Acta Psychiatrica Scandinavica. wileyonlinelibrary. 108 (1): 70–72. doi:10.1034/j.1600-0447.2003.00080.x. PMID 12807380.
- Mendhekar, D. N.; Gupta, D.; Girotra, V. (1 July 2003). "Sertraline‐induced hypomania: a genuine side‐effect". Department of Psychiatry. DCBI. 108 (1): 70–4. doi:10.1034/j.1600-0447.2003.00080.x. PMID 12807380.
- "Medications used when high (hypomania/mania)". bipolaruk. Retrieved 2019-07-03.
- Emanuel Mendel (1881) Die Manie, p. 36: "Hypomanie", Urban & Schwarzenberg, Vienna and Leipzig (in German)
- Thomas, P (April 2004). "The many forms of bipolar disorder: a modern look at an old illness". Journal of Affective Disorders. 79: 3–8. doi:10.1016/j.jad.2004.01.001. PMID 15121341.
- Baldwin et al. (1902) Dictionary of Philosophy and Psychology, p. 101: "Monomania", Macmillan: New York; London
- James Johnson, M.D., Ed. (1843) "Notices of Some New Works: Dr.H. Johnson on Mental Disorders", The Medical-Chirurgical Review, Vol. 39, p. 460: Hypomania
- Henry Johnson (1843) On the Arrangement and Nomenclature of Mental Disorders, Longmans, London, OCLC 706786581
- Edward Shorter (2005) A Historical Dictionary of Psychiatry, p.132, Oxford University Press, US ISBN 978-0-19803-923-5
External links
| Classification | |
|---|---|
| External resources |