Herpes esophagitis
Herpes esophagitis is a viral infection of the esophagus caused by Herpes simplex virus (HSV).
| Herpes esophagitis | |
|---|---|
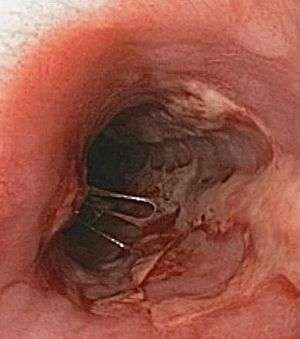 | |
| Endoscopic image of Herpes esophagitis | |
| Specialty | Infectious disease, gastroenterology |
While the disease most often occurs in immunocompromised patients, including post-chemotherapy, immunosuppression with organ transplants[1] and in AIDS,[2] herpes esophagitis can also occur in immunocompetent individuals.[3]
Signs and symptoms
People with herpes esophagitis experience pain with eating and trouble swallowing. Other symptoms can include food impaction,[4] hiccups,[5] weight loss, fever,[3] and on rare occasions upper gastrointestinal bleeding as noted in the image above[6] and tracheoesophageal fistula.[7] Frequently one can see herpetiform lesions in the mouth and lips.
Diagnosis
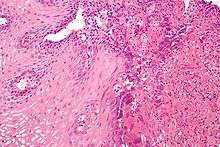
Upper Endoscopy often reveals ulcers throughout the esophagus with intervening normal-appearing mucosa. In severe cases the ulcers can coalesce and on rare occasions have a black appearance known as black esophagus.[8] While the diagnosis of herpes esophagitis can be inferred clinically it can only be accurately diagnosed through endoscopically obtained biopsies with microscopic evaluation by a pathologist finding the appropriate inclusion bodies and diagnostic immunochemical staining.[9] False negative findings may occur if biopsies are taken from the ulcer rather than from the margin of the ulcer as the inclusion particles are to be found in viable epithelial cells. Viral tissue culture represents the most accurate means of diagnosing the precise cause.
Differential diagnosis
CMV, VZV as well as HIV infections of the esophagus can have a similar presentation. Tissue culture is the most accurate means of distinguishing between the different viral causes.[10] Caustic esophagitis, pill-induced esophagitis as well as yeast esophagitis can have a similar clinical presentation.
Prevention
Herpes simplex virus is commonly found in humans, yet uncommonly results in systemic manifestations. Suppression of HIV with antiretroviral medications, careful monitoring of immunosuppressive medications are important means of prevention. Antiviral prophylaxis such as daily acyclovir in immunocompromised individuals may be considered.
Treatment
Antivirals such as acyclovir, famciclovir, or valacyclovir may be used. Intravenous acyclovir is reserved for individuals who cannot swallow due to the pain, individuals with other systemic manifestations of herpes or severely immunocompromised individuals.
References
- Miller GG, Dummer JS (April 2007). "Herpes simplex and varicella zoster viruses: forgotten but not gone". Am. J. Transplant. 7 (4): 741–7. doi:10.1111/j.1600-6143.2006.01718.x. PMID 17391119.
- McBane RD, Gross JB (1991). "Herpes esophagitis: clinical syndrome, endoscopic appearance, and diagnosis in 23 patients". Gastrointest. Endosc. 37 (6): 600–3. doi:10.1016/s0016-5107(91)70862-6. PMID 1756917.
- Kato S, Yamamoto R, Yoshimitsu S, et al. (2005). "Herpes simplex esophagitis in the immunocompetent host". Dis. Esophagus. 18 (5): 340–4. doi:10.1111/j.1442-2050.2005.00510.x. PMID 16197537.
- Marshall JB, Smart JR, Elmer C, Lillich MA, Diaz-Arias AA (September 1992). "Herpes esophagitis causing an unsuspected esophageal food bolus impaction in an institutionalized patient". J. Clin. Gastroenterol. 15 (2): 179–80. doi:10.1097/00004836-199209000-00032. PMID 1328357.
- Mulhall BP, Nelson B, Rogers L, Wong RK (May 2003). "Herpetic esophagitis and intractable hiccups (singultus) in an immunocompetent patient". Gastrointest. Endosc. 57 (6): 796–7. doi:10.1067/mge.2003.212. PMID 12739568.
- Takeno M, Adachi H, Nakahama T, Inagaki Y, Morimoto H, Watanabe K (August 2002). "[Herpes esophagitis presenting upper gastrointestinal bleeding: report of a case]". Nihon Shokakibyo Gakkai Zasshi (in Japanese). 99 (8): 935–40. PMID 12229166.
- Obrecht WF, Richter JE, Olympio GA, Gelfand DW (November 1984). "Tracheoesophageal fistula: a serious complication of infectious esophagitis". Gastroenterology. 87 (5): 1174–9. doi:10.1016/S0016-5085(84)80082-7. PMID 6592123.
- Nagri S, Hwang R, Anand S, Kurz J (February 2007). "Herpes simplex esophagitis presenting as acute necrotizing esophagitis ("black esophagus") in an immunocompetent patient". Endoscopy. 39 (Suppl 1): E169. doi:10.1055/s-2007-966619. PMID 17614059.
- Bennett WE, Tarr PI (January 2009). "Enteric infections and diagnostic testing". Curr. Opin. Gastroenterol. 25 (1): 1–7. doi:10.1097/MOG.0b013e32831ba094. PMID 19114768.
- Meinhard Classen; Guido N. J. Tytgat; M.D. Ph.D.; Charles J. Lightdale (2010). Gastroenterological Endoscopy. Thieme. pp. 490–. ISBN 978-3-13-125852-6. Retrieved 26 June 2010.