Fecal impaction
A fecal impaction is a solid, immobile bulk of feces that can develop in the rectum as a result of chronic constipation. A related term is fecal loading which refers to a large volume of stool in the rectum of any consistency.[1]
| Fecal impaction | |
|---|---|
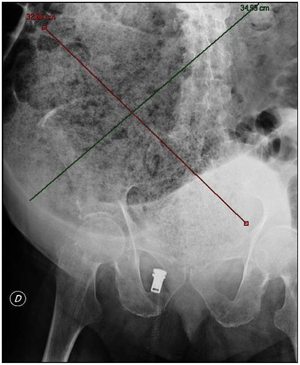 | |
| Plain abdominal X-ray showing a huge fecal impaction extending from the pelvis upwards to the left subphrenic space and from the left towards the right flank, measuring over 40 cm in length and 33 cm in width. | |
| Specialty | Gastroenterology |
Signs and symptoms
Symptoms include chronic constipation. There can be fecal incontinence and paradoxical overflow diarrhea (encopresis) as liquid stool passes around the obstruction. Complications may include necrosis and ulcers of the rectal tissue. Abdominal pain and bloating could also be present depending on the severity of the condition. Loss of appetite can also occur.
Causes
There are many possible causes; for example, physical inactivity, not eating enough (particularly of fiber), not drinking enough water, and holding in bowel movements.
Medications such as opioid pain relievers (fentanyl, buprenorphine, methadone, codeine, oxycodone, hydrocodone, morphine, hydromorphone, etc.) and certain sedatives that reduce intestinal movement may cause fecal matter to become too large, hard and/or dry to expel.
Specific conditions, such as irritable bowel syndrome, neurological disorders, paralytic ileus, gastroparesis, diabetes, dehydration, enlarged prostate gland, distended colon, ingested foreign object, inflammatory bowel diseases such as crohn's disease and colitis, and autoimmune diseases such as amyloidosis, celiac disease, lupus, and scleroderma can cause constipation. Hypothyroidism can cause chronic constipation because of sluggish, slower, or weaker colon contractions. Iron supplements or increased blood calcium levels are also potential causes. Spinal cord injury is a common cause of constipation, due to ileus.
Manual removal of a fecal impaction is often required with obese patients in traction, after a barium enema, and in poorly hydrated older adults.
Prevention
Reducing opiate-based medication (when possible, tolerable, and safe; prescription medication changes should be done under the supervision of a physician), and adequate intake of liquids (water) and dietary fiber and daily exercise.
Treatment
The treatment of fecal impaction requires both the remedy of the impaction and treatment to prevent future recurrences. Decreased motility of the colon results in dry, hard stools that in the case of fecal impaction become compacted into a large, hard mass of stool that cannot be expelled from the rectum.
Various methods of treatment attempt to remove the impaction by softening the stool, lubricating the stool, or breaking it into pieces small enough for removal. Enemas and osmotic laxatives can be used to soften the stool by increasing the water content until it is soft enough to be expelled. Osmotic laxatives such as magnesium citrate work within minutes - 8 hours for onset of action, and even then they may not be sufficient to expel the stool.
Osmotic laxatives can cause cramping and even severe pain as the patient's attempts to evacuate the contents of the rectum are blocked by the fecal mass. Polyethylene glycol (PEG 3350) may be used to increase the water content of the stool without cramping; however, since it may take 24 to 48 hours for it to take effect, it is not well suited to cases where the impaction needs to be removed immediately due to risk of complications or severe pain. Enemas (such as hyperosmotic saline) and suppositories (such as glycerine suppositories) work by increasing water content and stimulating peristalsis to aid in expulsion, and both work much more quickly than oral laxatives.
Because enemas work in 2–15 minutes, they do not allow sufficient time for a large fecal mass to soften. Even if the enema is successful at dislodging the impacted stool, the impacted stool may remain too large to be expelled through the anal canal. Mineral oil enemas can assist by lubricating the stool for easier passage. In cases where enemas fail to remove the impaction, polyethylene glycol can be used to attempt to soften the mass over 24–48 hours, or if immediate removal of the mass is needed, manual disimpaction may be used. Manual disimpaction may be performed by lubricating the anus and using one gloved finger with a scoop-like motion to break up the fecal mass. Most often manual disimpaction is performed without general anaesthesia, although sedation may be used. In more involved procedures, general anaesthesia may be used, although the use of general anaesthesia increases the risk of damage to the anal sphincter. If all other treatments fail, surgery may be necessary.
Individuals who have had one fecal impaction are at high risk of future impactions. Therefore, preventive treatment should be instituted in patients following the removal of the mass. Increasing dietary fiber, increasing fluid intake, exercising daily, and attempting regularly to defecate every morning after eating should be promoted in all patients.
Often underlying medical conditions cause fecal impactions; these conditions should be treated to reduce the risk of future impactions. Many types of medications (most notably opioid pain medications, such as codeine) reduce motility of the colon, increasing the likelihood of fecal impactions. If possible, alternate medications should be prescribed that avoid the side effect of constipation.
Given that all opioids can cause constipation,[2] it is recommended that any patient placed on opioid pain medications be given medications to prevent constipation before it occurs. Daily medications can also be used to promote normal motility of the colon and soften stools. Daily use of laxatives or enemas should be avoided by most individuals as it can cause the loss of normal colon motility. However, for patients with chronic complications, daily medication under the direction of a physician may be needed.
Polyethylene glycol 3350 can be taken daily to soften the stools without the significant risk of adverse effects that are common with other laxatives. In particular, stimulant laxatives should not be used frequently because they can cause dependence in which an individual loses normal colon function and is unable to defecate without taking a laxative.[3] Frequent use of osmotic laxatives should be avoided as well as they can cause electrolyte imbalances.
Fecaloma
A fecaloma is a more extreme form of fecal impaction, giving the accumulation an appearance of a tumor.[4]
A fecaloma can develop as the fecal matter gradually stagnates and accumulates in the intestine and increases in volume until the intestine becomes deformed.[5] It may occur in chronic obstruction of stool transit, as in megacolon[6] and chronic constipation. Some diseases, such as Chagas disease, Hirschsprung's disease and others damage the autonomic nervous system in the colon's mucosa (Auerbach's plexus) and may cause extremely large or "giant" fecalomas, which must be surgically removed (disimpaction). Rarely, a fecalith will form around a hairball (Trichobezoar), or other hygroscopic or desiccant nucleus.
It can be diagnosed by:
Distal or sigmoid, fecalomas can often be disimpacted digitally or by a catheter which carries a flow of disimpaction fluid (water or other solvent or lubricant). Surgical intervention in the form of sigmoid colectomy[8] or proctocolectomy and ileostomy[9] may be required only when all conservative measures of evacuation fail. Attempts at removal can have severe and even lethal effects, such as the rupture of the colon wall by catheter or an acute angle of the fecaloma (stercoral perforation), followed by sepsis. It may also lead to stercoral perforation, a condition characterized by bowel perforation due to pressure necrosis from a fecal mass or fecaloma.[10][11]
See also
- Impaction (animals)
- Aerosol impaction
- Dental impaction
References
- (UK), National Collaborating Centre for Acute Care (2007). Faecal incontinence the management of faecal incontinence in adults. London: National Collaborating Centre for Acute Care (UK). ISBN 978-0-9549760-4-0.
- Opioid#Constipation
- Joo JS, Ehrenpreis ED, Gonzalez L, et al. (June 1998). "Alterations in colonic anatomy induced by chronic stimulant laxatives: the cathartic colon revisited". Journal of Clinical Gastroenterology. 26 (4): 283–6. doi:10.1097/00004836-199806000-00014. PMID 9649012.
- "Fecaloma". Farlex medical dictionary. Retrieved 2018-01-04.
- Yucel, AF; Akdogan, RA; Gucer, H (February 2012). "A giant abdominal mass: fecaloma". Clinical Gastroenterology and Hepatology. 10 (2): e9–e10. doi:10.1016/j.cgh.2011.06.030. PMID 21749849.
- Rajagopal, A; Martin, J (June 2002). "Giant fecaloma with idiopathic sigmoid megacolon: report of a case and review of the literature". Diseases of the Colon and Rectum. 45 (6): 833–5. doi:10.1007/s10350-004-6306-x. PMID 12072639.
- Fagelman, D; Warhit, JM; Reiter, JD; Geiss, AC (June 1984). "CT diagnosis of fecaloma". Journal of Computer Assisted Tomography. 8 (3): 559–61. doi:10.1097/00004728-198406000-00040. PMID 6725706.
- Garisto, JD; Campillo, L; Edwards, E; Harbour, M; Ermocilla, R (5 February 2009). "Giant fecaloma in a 12-year-old-boy: a case report". Cases Journal. 2 (1): 127. doi:10.1186/1757-1626-2-127. PMC 2642792. PMID 19196473.
- Altomare, DF; Rinaldi, M; Sallustio, PL; Armenise, N (March 2009). "Giant fecaloma in an adult with severe anal stricture caused by anal imperforation treated by proctocolectomy and ileostomy: report of a case". Diseases of the Colon and Rectum. 52 (3): 534–7. doi:10.1007/DCR.0b013e318199db36. PMID 19333059.
- Kumar, P; Pearce, O; Higginson, A (January 2011). "Imaging manifestations of faecal impaction and stercoral perforation". Clinical Radiology. 66 (1): 83–8. doi:10.1016/j.crad.2010.08.002. PMID 21147303.
- Hsiao, TF; Chou, YH (January 2010). "Stercoral perforation of colon: a rare but important mimicker of acute appendicitis". The American Journal of Emergency Medicine. 28 (1): 112.e1–2. doi:10.1016/j.ajem.2009.02.024. PMID 20006219.
Further reading
- Wrenn K (September 1989). "Fecal impaction". The New England Journal of Medicine. 321 (10): 658–62. doi:10.1056/NEJM198909073211007. PMID 2671728.
- Dugdale, David C. (January 31, 2011). "Fecal impaction". A.D.A.M., Inc.
- Gattuso JM, Kamm MA, Halligan SM, Bartram CI (April 1996). "The anal sphincter in idiopathic megarectum: effects of manual disimpaction under general anesthetic". Diseases of the Colon and Rectum. 39 (4): 435–9. doi:10.1007/bf02054060. PMID 8878505.
External links
| Classification | |
|---|---|
| External resources |