Neisseria meningitidis
Neisseria meningitidis, often referred to as meningococcus, is a Gram-negative bacterium that can cause meningitis and other forms of meningococcal disease such as meningococcemia, a life-threatening sepsis. The bacterium is referred to as a coccus because it is round, and more specifically, diplococcus because of its tendency to form pairs. About 10% of adults are carriers of the bacteria in their nasopharynx.[1] As an exclusively human pathogen it is the main cause of bacterial meningitis in children and young adults, causing developmental impairment and death in about 10% of cases. It causes the only form of bacterial meningitis known to occur epidemically, mainly in Africa and Asia. It occurs worldwide in both epidemic and endemic form.[2] N. meningitidis is spread through saliva and respiratory secretions during coughing, sneezing, kissing, chewing on toys and even through sharing a source of fresh water. It has also been reported to be transmitted through oral sex and cause urethritis in men.[3] It infects its host cells by sticking to them with long thin extensions called pili and the surface-exposed proteins Opa and Opc and has several virulence factors.
| Neisseria meningitidis | |
|---|---|
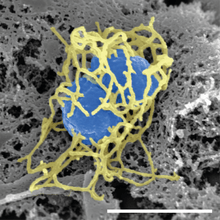 | |
| Scanning electron micrograph of a single N. meningitidis cell (colorized in blue) with its adhesive pili (colorized in yellow). The scale bar corresponds to 1 µm. | |
| Scientific classification | |
| Domain: | Bacteria |
| Phylum: | Proteobacteria |
| Class: | Betaproteobacteria |
| Order: | Neisseriales |
| Family: | Neisseriaceae |
| Genus: | Neisseria |
| Species: | N. meningitidis |
| Binomial name | |
| Neisseria meningitidis Albrecht & Ghon 1901 | |
Signs and symptoms
Meningococcus can cause meningitis and other forms of meningococcal disease.[4] It initially produces general symptoms like fatigue, fever, and headache and can rapidly progress to neck stiffness, coma and death in 10% of cases. Petechiae occur in about 50% of cases. Chance of survival is highly correlated with blood cortisol levels, and so a reduction in cortisol can be used to determine likelihood of patient mortality.[5] Symptoms of meningococcal meningitis are easily confused with those caused by other bacteria, such as Haemophilus influenzae and Streptococcus pneumoniae.[6][7] Suspicion of meningitis is a medical emergency and immediate medical assessment is recommended. Current guidance in the United Kingdom is that if a case of meningococcal meningitis or septicaemia (infection of the blood) is suspected, intravenous antibiotics should be given and the ill person admitted to the hospital.[8] This means that laboratory tests may be less likely to confirm the presence of Neisseria meningitidis as the antibiotics will dramatically lower the number of bacteria in the body. The UK guidance is based on the idea that the reduced ability to identify the bacteria is outweighed by reduced chance of death.
Septicaemia caused by Neisseria meningitidis has received much less public attention than meningococcal meningitis even though septicaemia has been linked to infant deaths.[9] Meningococcal septicaemia typically causes a purpuric rash, that does not lose its color when pressed with a glass slide ("non-blanching") and does not cause the classical symptoms of meningitis. This means the condition may be ignored by those not aware of the significance of the rash. Septicaemia carries an approximate 50% mortality rate over a few hours from initial onset.
Other severe complications include Waterhouse–Friderichsen syndrome, a massive, usually bilateral, hemorrhage into the adrenal glands caused by fulminant meningococcemia, adrenal insufficiency, and disseminated intravascular coagulation.[7]
Not all instances of a purpura-like rash are due to meningococcal septicaemia; other possible causes, such as idiopathic thrombocytopenic purpura (ITP; a platelet disorder) and Henoch–Schönlein purpura, also need prompt investigation.
Microbiology
N. meningitidis is a Gram-negative diplococcus since it has an outer and inner membranes with a thin layer of peptidoglycan in between. It is 0.6–1.0 micrometers in size. It tests positive for the enzyme cytochrome c oxidase.[10]
Habitat
N. meningitidis is a part of the normal nonpathogenic flora in the nasopharynx of up to 5–15% of adults.[11] It colonizes and infects only humans, and has never been isolated from other animals. This is thought to stem from the bacterium's inability to get iron from sources other than human transferrin and lactoferrin.[6]
Subtypes
Disease-causing strains are classified according to the antigenic structure of their polysaccharide capsule.[12] Serotype distribution varies markedly around the world.[13] Among the 13 identified capsular types of N. meningitidis, six (A, B, C, W135, X, and Y) account for most disease cases worldwide.[14] Type A has been the most prevalent in Africa and Asia, but is rare/practically absent in North America. In the United States, serogroup B is the predominant cause of disease and mortality, followed by serogroup C. The multiple subtypes have hindered development of a universal vaccine for meningococcal disease.
Pathogenesis
Virulence
Lipooligosaccharide (LOS) is a component of the outer membrane of N. meningitidis. This acts as an endotoxin and is responsible for septic shock and hemorrhage due to the destruction of red blood cells.[15] Other virulence factors include a polysaccharide capsule which prevents host phagocytosis and aids in evasion of the host immune response; fimbriae mediate attachment of the bacterium to the epithelial cells of the nasopharynx.[16][17] It infects the cell by sticking to it mainly with long thin extensions called pili and the surface-exposed proteins Opa and Opc.[18] Meningococci produce an IgA protease, an enzyme that cleaves IgA class antibodies and thus allows the bacteria to evade a subclass of the humoral immune system.
A hypervirulent strain was discovered in China. Its impact is yet to be determined.[7]
Complement inhibition
Factor H binding protein (fHbp) that is exhibited in N. meningitidis and some commensal species is the main inhibitor of the alternative complement pathway. fHbp protects meningococci from complement-mediated death in human serum experiments, but has also been shown to protect meningococci from antimicrobial peptides in vitro. Factor H binding protein is key to the pathogenesis of N. meningitidis, and is, therefore, important as a potential vaccine candidate.[19] Porins are also an important factor for complement inhibition for both pathogenic and commensal species. Porins are important for nutrient acquisition. Porins are also recognized by TLR2, they bind complement factors (C3b, C4b, factor H, and C4bp (complement factor 4b-binding protein)). Cooperation with pili for CR3-mediated internalization is another function of porins. Ability to translocate into host cells and modulate reactive oxygen species production and apoptosis is made possible by porins, as well. Strains of the same species can express different porins.
Genome
At least 8 complete genomes of Neisseria meningitidis strains have been determined which encode about 2,100 to 2,500 proteins.[20]
The genome of strain MC58 (serogroup B) has 2,272,351-base pairs. When sequenced in 2000, it was found to contain 2158 open reading frames (ORFs). Of these, a biological function was predicted for 1158 (53.7%). There were three major islands of horizontal DNA transfer found. Two encode proteins involved in pathogenicity. The third island only codes for hypothetical proteins. They also found more genes that undergo phase variation than any pathogen then known. Phase variation is a mechanism that helps the pathogen to evade the immune system of the host.[21]
The genome size of strain H44/76 is 2.18 Mb, and encodes 2,480 open reading frames (ORFs), compared to 2.27 Mb and 2,465 ORFs for MC58.[20] Both strains have a GC content of 51.5%.[20] A comparison with MC58 showed that four genes are uniquely present in H44/76 and nine genes are only present in MC58. Of all ORFs in H44/76, 2,317 (93%) show more than 99% sequence identity.[20]
The complete genome sequence of strain NMA510612 (serogroup A) consists of one circular chromosome with a size of 2,188,020 bp, and the average GC content is 51.5%. The chromosome is predicted to possess 4 rRNA operons, 163 insertion elements (IS), 59 tRNAs, and 2,462 ORFs.[22]
Genetic transformation
Genetic transformation is the process by which a recipient bacterial cell takes up DNA from a neighboring cell and integrates this DNA into the recipient’s genome by recombination. In N. meningitidis, DNA transformation requires the presence of short DNA sequences (9–10 mers residing in coding regions) of the donor DNA. These sequences are called DNA uptake sequences (DUSs). Specific recognition of these sequences is mediated by a type IV pilin.[23] In N. meningitidis DUSs occur at a significantly higher density in genes involved in DNA repair and recombination (as well as in restriction-modification and replication) than in other annotated gene groups. The over-representation of DUS in DNA repair and recombination genes may reflect the benefit of maintaining the integrity of the DNA repair and recombination machinery by preferentially taking up genome maintenance genes, that could replace their damaged counterparts in the recipient cell.[24]
N. meningititis colonizes the nasopharyngeal mucosa, which is rich in macrophages. Upon their activation, macrophages produce superoxide (O2¯) and hydrogen peroxide (H2O2). Thus N. meningitidis is likely to encounter oxidative stress during its life cycle.[25] Consequently, an important benefit of genetic transformation to N. meningitidis may be the maintenance of the recombination and repair machinery of the cell that removes oxidative DNA damages such as those caused by reactive oxygen. This is consistent with the more general idea that transformation benefits bacterial pathogens by facilitating repair of DNA damages produced by the oxidative defenses of the host during infection.[26]
Diagnosis

With a fatality risk approaching 15% within 12 hours of infection, it is crucial to initiate testing as quickly as possible, but not to wait for the results before initiating antibiotic therapy.
A small amount of cerebrospinal fluid (CSF) is sent to the laboratory as soon as possible for analysis. The diagnosis is suspected, when Gram-negative diplococci are seen on Gram stain of a centrifuged sample of CSF; sometimes they are located inside white blood cells. The microscopic identification takes around 1–2 hours after specimen arrival in the laboratory.[4]
The gold standard of diagnosis is microbiological isolation of N. meningitidis by growth from a sterile body fluid, which could be CSF or blood.[7] Diagnosis is confirmed when the organism has grown, most often on a chocolate agar plate, but also on Thayer-Martin agar. To differentiate any bacterial growth from other species a small amount of a bacterial colony is tested for oxidase, catalase for which all clinically relevant Neisseria show a positive reaction, and the carbohydrates maltose, sucrose, and glucose, in which N. meningitidis will ferment that is, utilize the glucose and maltose. Finally, serology determines the subgroup of the N. meningitidis, which is important for epidemiological surveillance purposes; this may often only be done in specialized laboratories.
The above tests take a minimum of 48–72 hours turnaround time for growing the organism, and up to a week more for serotyping. Growth can and often does fail, either because antibiotics have been given preemptively, or because specimens have been inappropriately transported, as the organism is extremely susceptible to antibiotics and fastidious in its temperature, CO
2 and growth medium requirements.
Polymerase chain reaction (PCR) tests where available, mostly in industrialized countries, have been increasingly used; PCR can rapidly identify the organism, and works even after antibiotics have been given.[7]
Prevention
All recent contacts of the infected patient over the 7 days before onset should receive medication to prevent them from contracting the infection. This especially includes young children and their child caregivers or nursery-school contacts, as well as anyone who had direct exposure to the patient through kissing, sharing utensils, or medical interventions such as mouth-to-mouth resuscitation. Anyone who frequently ate, slept or stayed at the patient's home during the 7 days before the onset of symptom, or those who sat beside the patient on an airplane flight or classroom for 8 hours or longer, should also receive chemoprophylaxis. The agent of choice is usually oral rifampicin for a few days.[7]
Receiving a dose of the Meningococcal vaccine before traveling to a country in the "meningitis belt" or having a booster meningitis vaccine, normally five years apart could prevent someone from getting an infection from the pathogen.[27]
Vaccination
United States
A number of vaccines are available in the U.S. to prevent meningococcal disease. Some of the vaccines cover serogroup B, while others cover A, C, W, and Y.[28] A meningococcal polysaccharide vaccine (MPSV4) has been available since the 1970s and is the only meningococcal vaccine licensed for people older than 55. MPSV4 may be used in people 2–55 years old if the MCV4 vaccines are not available or contraindicated. Two meningococcal conjugate vaccines (MCV4) are licensed for use in the U.S. The first conjugate vaccine was licensed in 2005, the second in 2010. Conjugate vaccines are the preferred vaccine for people 2 through 55 years of age. It is indicated in those with impaired immunity, such as nephrotic syndrome or splenectomy. The Centers for Disease Control and Prevention (CDC) publishes information about who should receive meningococcal vaccine.[29]
In June 2012, the U.S. Food and Drug Administration (FDA) approved a combination vaccine against two types of meningococcal diseases and Hib disease for infants and children 6 weeks to 18 months old. The vaccine, Menhibrix, was designed to prevent disease caused by Neisseria meningitidis serogroups C and Y, and Haemophilus influenzae type b (Hib). It was the first meningococcal vaccine that could be given to infants as young as six weeks old.[30]
In October 2014 the FDA approved the first vaccine effective against serogroup B, named Trumenba, for use in 10- to 25-year-old individuals.[31]
Africa
In 2010, the Meningitis Vaccine Project introduced a vaccine called MenAfriVac in the African meningitis belt. It was made by generic drug maker Serum Institute of India and cost 50 U.S. cents per injection. Beginning in Burkina Faso in 2010, it has been given to 215 million people across Benin, Cameroon, Chad, Ivory Coast, Ethiopia, Ghana, Mali, Niger, Mauritania, Nigeria, Senegal, Sudan, Togo and Gambia.[32] The vaccination campaign has resulted in near-elimination of serogroup A meningitis from the participating countries.[33]
Treatment
Persons with confirmed N. meningitidis infection should be hospitalized immediately for treatment with antibiotics. Because meningococcal disease can disseminate very rapidly, a single dose of intramuscular antibiotic is often given at the earliest possible opportunity, even before hospitalization, if disease symptoms look suspicious enough.[7] Third-generation cephalosporin antibiotics (i.e. cefotaxime, ceftriaxone) should be used to treat a suspected or culture-proven meningococcal infection before antibiotic susceptibility results are available.[34] Empirical treatment should also be considered if a lumbar puncture, to collect CSF for laboratory testing, cannot be done within 30 minutes of admission to hospital.[35][36] Antibiotic treatment may affect the results of microbiology tests, but a diagnosis may be made on the basis of blood-cultures and clinical examination.[37]
Epidemiology
N. meningitidis is a major cause of illness, developmental impairment and death during childhood in industrialized countries and has been responsible for epidemics in Africa and in Asia. Every year, about 2,500 to 3,500 people become infected with N. meningitidis in the US, with a frequency of about 1 in 100,000. Children younger than 5 years are at greatest risk, followed by teenagers of high school age. Rates in the African meningitis belt were as high as 1 in 1,000 to 1 in 100[7] before introduction of a vaccine in 2010. The incidence of meningococcal disease is highest among infants (children younger than 1-year-old) whose immune system is relatively immature. In industrialized countries there is a second peak of incidence in young adults, who are congregating closely, living in dormitories or smoking.[38] Vaccine development is ongoing.[39] It is spread through saliva and other respiratory secretions during coughing, sneezing, kissing, and chewing on toys. Inhalation of respiratory droplets from a carrier which may be someone who is themselves in the early stages of disease can transmit the bacteria. Close contact with a carrier is the predominant risk factor. Other risk factors include a weakened general or local immune response, such as a recent upper respiratory infection, smoking, and complement deficiency. The incubation period is short, from 2 to 10 days. In susceptible individuals, N. meningitidis may invade the bloodstream and cause a systemic infection, sepsis, disseminated intravascular coagulation, breakdown of circulation, and septic shock.
History
In 1884 Ettore Marchiafava and Angelo Celli first observed the bacterium inside cells in the cerebral spinal fluid (CSF).[40] In 1887 Anton Weichselbaum isolated the bacterium from the CSF of patients with bacterial meningitis.[41] He named the bacterium Diplococcus intracellularis meningitidis.[40]
See also
- DNA uptake sequence DNA taken up by Neisseria
- NmVac4-A/C/Y/W-135 polysaccharide vaccine
- Sara Branham Matthews microbiologist
- Shwartzman phenomenon
- Sepsis
References
- Hitchcock P.J., Robinson E.N. (Jr.) and McGee Z.A., "Neisseriae: Gonococcus and Meningococcus", chap. 14 in Schaechter M., Medoff G. and Eisenstein B.I., Mechanisms of Microbial Disease, 2nd Ed., Baltimore, Williams & Wilkins, 1993., p.231.
- "CDC Works 24/7". Centers for Disease Control and Prevention. 2018-10-11. Retrieved 2016-04-17.
- "Notes from the Field: Increase in Neisseria meningitidis–Associated Urethritis Among Men at Two Sentinel Clinics — Columbus, Ohio, and Oakland County, Michigan, 2015". CDC. 2016-06-03. Retrieved 2018-12-24.
- Ryan, K.J.; Ray, C.G., eds. (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. pp. 329–333. ISBN 978-0-8385-8529-0.
- Critical Care Medicine. 27(10):2257-2261, OCTOBER 1999
- Pollard & Maiden 2001, p. 1
- Mola SJ, Nield LS, Weisse ME (February 27, 2008). "Treatment and Prevention of N. meningitidis Infection". Infections in Medicine.(subscription required)
- Health Protection Agency Meningococcus Forum (August 2006). "Guidance for public health management of meningococcal disease in the UK".
- Pollard, Andrew J.; Maiden, Martin C.J. (2001). Meningococcal Vaccines. Humana. ISBN 978-0-89603-801-1.CS1 maint: ref=harv (link)
- "Neisseria meningitidis". Centers for Disease Control and Prevention. 24 October 2008.
- "Neisseria meningitidis". Brown University. Archived from the original on 10 November 2009. Retrieved 22 October 2009.
- Centers for Disease Control and Prevention (CDC), Meningococcal Disease, Epidemiology and Prevention of Vaccine-Preventable Diseases, 13th Ed., April, 2015.
- "Archived copy". Archived from the original on 2013-06-06. Retrieved 2013-01-03.CS1 maint: archived copy as title (link)
- Harrison, Lee H. (2010). "Epidemiological Profile of Meningococcal Disease in the United States". Clinical Infectious Diseases. 50 (Suppl 2): S37–S44. doi:10.1086/648963. PMC 2820831. PMID 20144015.
- Griffiss JM, Schneider H, Mandrell RE, Yamasaki R, Jarvis GA, Kim JJ, Gibson BW, Hamadeh R, Apicella MA (1988). "Lipooligosaccharides: the principal glycolipids of the neisserial outer membrane". Rev Infect Dis. 10 Suppl 2: S287–95. doi:10.1093/cid/10.supplement_2.s287. PMID 2460911.
- Jarrell, K., ed. (2009). Pili and Flagella: Current Research and Future Trends. Caister Academic. ISBN 978-1-904455-48-6.
- Ullrich, M., ed. (2009). Bacterial Polysaccharides: Current Innovations and Future Trends. Caister Academic. ISBN 978-1-904455-45-5.
- Hall, DJ; Griffiths, NJ; Borodina, E; Mumtaz, V (2010). "Cellular and molecular biology of Neisseria meningitidis colonization and invasive disease". Clinical Science. 118 (9): 547–564. doi:10.1042/CS20090513. PMC 2830671. PMID 20132098.
- "404 | Meningitis Research Foundation".
- Piet, J. R.; Huis in 't Veld RA; Van Schaik, B. D.; Van Kampen, A. H.; Baas, F; Van De Beek, D; Pannekoek, Y; Van Der Ende, A (2011). "Genome sequence of Neisseria meningitidis serogroup B strain H44/76". Journal of Bacteriology. 193 (9): 2371–2. doi:10.1128/JB.01331-10. PMC 3133077. PMID 21378179.
- Tettelin, H.; Saunders, N.; Heidelberg, J.; Jeffries, A.; Nelson, K.; Eisen, J.; Ketchum, K.; Hood, D.; Peden, J.; Dodson, R. J.; Nelson, W. C.; Gwinn, M. L.; Deboy, R.; Peterson, J. D.; Hickey, E. K.; Haft, D. H.; Salzberg, S. L.; White, O.; Fleischmann, R. D.; Dougherty, B. A.; Mason, T.; Ciecko, A.; Parksey, D. S.; Blair, E.; Cittone, H.; Clark, E. B.; Cotton, M. D.; Utterback, T. R.; Khouri, H.; Qin, H. (2000). "Complete genome sequence of Neisseria meningitidis serogroup B strain MC58". Science. 287 (5459): 1809–1815. Bibcode:2000Sci...287.1809.. doi:10.1126/science.287.5459.1809. PMID 10710307.
- Zhang, Y; Yang, J; Xu, L; Zhu, Y; Liu, B; Shao, Z; Zhang, X; Jin, Q (2014). "Complete Genome Sequence of Neisseria meningitidis Serogroup a Strain NMA510612, Isolated from a Patient with Bacterial Meningitis in China". Genome Announcements. 2 (3): e00360–14. doi:10.1128/genomeA.00360-14. PMC 4014685. PMID 24812217.
- Cehovin A, Simpson PJ, McDowell MA, Brown DR, Noschese R, Pallett M, Brady J, Baldwin GS, Lea SM, Matthews SJ, Pelicic V (February 2013). "Specific DNA recognition mediated by a type IV pilin". Proc. Natl. Acad. Sci. U.S.A. 110 (8): 3065–70. Bibcode:2013PNAS..110.3065C. doi:10.1073/pnas.1218832110. PMC 3581936. PMID 23386723.
- Davidsen T, Rødland EA, Lagesen K, Seeberg E, Rognes T, Tønjum T (2004). "Biased distribution of DNA uptake sequences towards genome maintenance genes". Nucleic Acids Res. 32 (3): 1050–8. doi:10.1093/nar/gkh255. PMC 373393. PMID 14960717.
- Dyet K, Moir J (February 2006). "Effect of combined oxidative and nitrosative stress on Neisseria meningitidis". Biochem. Soc. Trans. 34 (Pt 1): 197–9. doi:10.1042/BST0340197. PMID 16417521.
- Michod RE, Bernstein H, Nedelcu AM (May 2008). "Adaptive value of sex in microbial pathogens". Infect. Genet. Evol. 8 (3): 267–85. doi:10.1016/j.meegid.2008.01.002. PMID 18295550.
- "Meningococcal | Prevention | CDC". www.cdc.gov. 2017-07-24. Retrieved 2016-04-17.
- "Meningococcal Vaccination". U.S. Centers for Disease Control and Prevention. 2017-11-27. Retrieved 1 September 2016.
- "Menningococcal Vaccines – What You Need to Know" (PDF). Center for Disease Control and Prevention. 2008.
- "FDA approves new combination vaccine that protects children against two bacterial diseases" (Press release). FDA. 14 June 2012.
- "First vaccine approved by FDA to prevent serogroup B Meningococcal disease" (Press release). FDA. 29 October 2014.
- Kate Kelland (9 January 2015). "Tailor-made vaccine set to banish Africa's meningitis epidemics". Reuters. Thompson Reuters. Retrieved 10 January 2015.
- "Meningitis A Nearly Eliminated in Africa through Vaccination, Reaching more than 235 Million People". Immunization Africa. 22 February 2016. Retrieved 1 September 2016.
- Tunkel AR, Hartman BJ, Kaplan SL, Kaufman BA, Roos KL, Scheld WM, Whitley RJ (November 2004). "Practice guidelines for the management of bacterial meningitis". Clin Infect Dis. 39 (9): 1267–84. doi:10.1086/425368. PMID 15494903.
- Vallés J., Ferrer R. y Fernández-Viladrich P., "Bloodstream infections including Endocarditis and Meningitis", chap. 16 in Hendrik K.F, Van Saene H.K.F., Silvestri L. y Cal M.A. (eds.), Infection Control in the Intensive Care Unit,, Springer Science & Business Media, 2005, 639 pp. ISBN 88-470-0185-4.
- Acute Management of Suspected Meningococcal Disease Clinical Pathway Archived 2016-03-04 at the Wayback Machine, State of Queensland (Queensland Health) 2012.
- Coant P.N., Kornberg A.E., Duffy L.C., Dryja D.M., Hassan S.M. (1992). "Bloodculture results as determinants in the organism identification of bacterialmeningitis". Pediatr Emerg Care. 1992 (8): 200–205. doi:10.1097/00006565-199208000-00006. PMID 1381091.CS1 maint: multiple names: authors list (link)
- Genco, C.; Wetzler, L., eds. (2010). Neisseria: Molecular Mechanisms of Pathogenesis. Caister Academic. ISBN 978-1-904455-51-6.
- Baarda, Benjamin I.; Sikora, Aleksandra E. (2015). "Proteomics of Neisseria gonorrhoeae: the treasure hunt for countermeasures against an old disease". Frontiers in Microbiology. 6: 1190. doi:10.3389/fmicb.2015.01190. ISSN 1664-302X. PMC 4620152. PMID 26579097; Access provided by the University of Pittsburgh.
- Stephens DS (2009). "Biology and pathogenesis of the evolutionarily successful, obligate human bacterium Neisseria meningitidis". Vaccine. 27 (Suppl 2): B71–7. doi:10.1016/j.vaccine.2009.04.070. PMC 2712446. PMID 19477055.
- Bhalla, P; Manchanda, V; Gupta, S (2006). "Meningococcal disease: History, epidemiology, pathogenesis, clinical manifestations, diagnosis, antimicrobial susceptibility and prevention". Indian Journal of Medical Microbiology (Submitted manuscript). 24 (1): 7–19. doi:10.4103/0255-0857.19888. ISSN 0255-0857. PMID 16505549.
External links
- "Neisseria meningitidis". NCBI Taxonomy Browser. 487.
- Type strain of Neisseria meningitidis at BacDive - the Bacterial Diversity Metadatabase