Dihydropyrimidine dehydrogenase deficiency
Dihydropyrimidine dehydrogenase deficiency is an autosomal recessive[1] metabolic disorder in which there is absent or significantly decreased activity of dihydropyrimidine dehydrogenase, an enzyme involved in the metabolism of uracil and thymine.
| Dihydropyrimidine dehydrogenase deficiency | |
|---|---|
| Other names | DPD deficiency |
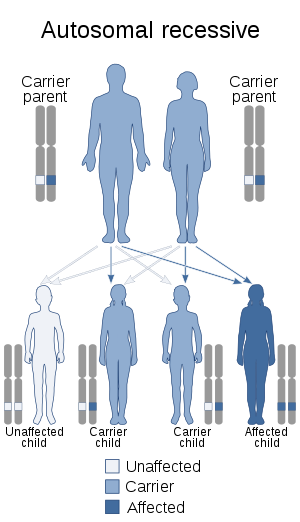 | |
| Dihydropyrimidine dehydrogenase deficiency has an autosomal recessive pattern of inheritance. | |
| Specialty | Medical genetics, endocrinology |
Individuals with this condition may develop life-threatening toxicity following exposure to 5-fluorouracil (5-FU), a chemotherapy drug that is used in the treatment of cancer.[2][3] Beside 5-FU, widely prescribed oral fluoropyrimidine capecitabine (Xeloda) could put DPD-deficient patients at risk of experiencing severe or lethal toxicities as well.[4][5]
Genetics
DPD deficiency is inherited in an autosomal recessive manner.[1] This means the defective gene responsible for the disorder is located on an autosome, and two copies of the defective gene (one inherited from each parent) are required in order to be born with the disorder. The parents of an individual with an autosomal recessive disorder both carry one copy of the defective gene, but usually do not experience any signs or symptoms of the disorder.
Diagnosis
Detecting DPD deficiency
A small number of genetic variants have been repeatedly associated with DPD deficiency, such as IVS14+1G>A mutation in intron 14 coupled with exon 14 deletion (a.k.a. DPYD*2A), 496A>G in exon 6; 2846A>T in exon 22 and T1679G (a.k.a. DPYD*13) in exon 13. However, testing patients for these allelic variants usually show high specificity (i.e., bearing the mutation means that severe toxicity will occur indeed) but very low sensitivity (i.e., not bearing the mutation does not mean that there is no risk for severe toxicities). Alternatively, phenotyping DPD using ex-vivo enzymatic assay or surrogate testing (i.e., monitoring physiological dihydrouracil to uracil ratio in plasma) has been presented as a possible upfront strategy to detect DPD deficiency. 5-FU test dose (i.e., preliminary administration of a small dose of 5-FU with pharmacokinetics evaluation) has been proposed as another possible alternative strategy to secure the use of fluoropyrimidine drugs.
Management
Epidemiology
Current research suggests that nearly 8% of the population has at least partial DPD deficiency. A diagnostics determination test for DPD deficiency is available and it is expected that with a potential 500,000 people in North America using 5-FU this form of testing will increase. The whole genetic events affecting the DPYD gene and possibly impacting on its function are far from being elucidated, and epigenetic regulations could probably play a major role in DPD deficiency. It seems that the actual incidence of DPD deficiency remains to be understood because it could depend on the very technique used to detect it. Screening for genetic polymorphisms affecting the DPYD gene usually identify less than 5% of patients bearing critical mutations, whereas functional studies suggest that up to 20% of patients could actually show various levels of DPD deficiency.
Women could be more at risk than men. It is more common among African-Americans than it is among Caucasians.[6]
References
- Diasio RB, Beavers TL, Carpenter JT (Jan 1988). "Familial deficiency of dihydropyrimidine dehydrogenase: biochemical basis for familial pyrimidinemia and severe 5-fluorouracil-induced toxicity". J Clin Invest. 81 (1): 47–51. doi:10.1172/JCI113308. PMC 442471. PMID 3335642.
- Van Kuilenburg AB (Mar 2006). "Screening for dihydropyrimidine dehydrogenase deficiency: to do or not to do, that's the question". Cancer Investigation. 24 (2): 215–217. doi:10.1080/07357900500524702. PMID 16537192.
- Lee A, Ezzeldin H, Fourie J, Diasio R (Aug 2004). "Dihydropyrimidine dehydrogenase deficiency: impact of pharmacogenetics on 5-fluorouracil therapy". Clinical Advances in Hematology & Oncology. 2 (8): 527–532. ISSN 1543-0790. PMID 16163233.
- Mercier C, Ciccolini J (Nov 2006). "Profiling dihydropyrimidine dehydrogenase deficiency in patients with cancer undergoing 5-fluorouracil/capecitabine therapy". Clinical Colorectal Cancer. 6 (4): 288–296. doi:10.3816/CCC.2006.n.047. ISSN 1533-0028. PMID 17241513.
- Mercier C, Ciccolini J (Dec 2007). "Severe or lethal toxicities upon capecitabine intake: is DPYD genetic polymorphism the ideal culprit?". Trends in Pharmacological Sciences. 28 (12): 597–598. doi:10.1016/j.tips.2007.09.009. PMID 18001850.
- Saif MW, Seller S, Diasio RB (Mar 2008). "Atypical toxicity associated with 5-Fluororacil in a DPD-deficient patient with pancreatic cancer. Is ethnicity a risk factor?". JOP. 9 (2): 226–9. PMID 18326935.
External links
| Classification | |
|---|---|
| External resources |
- Dihydropyrimidine dehydrogenase deficiency at NIH's Office of Rare Diseases