Genu varum
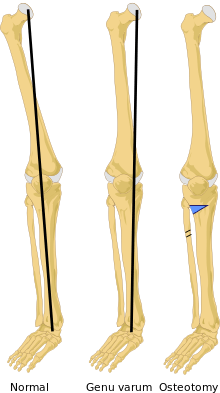
Genu varum (also called bow-leggedness, bandiness, bandy-leg, and tibia vara), is a varus deformity marked by (outward) bowing at the knee, which means that the lower leg is angled inward (medially) in relation to the thigh's axis, giving the limb overall the appearance of an archer's bow. Usually medial angulation of both lower limb bones (femur and tibia) is involved.
| Genu varum | |
|---|---|
| Other names | Bow-leggedness |
 | |
| X-Ray of the legs in a 2 year old child with rickets | |
| Specialty | Medical genetics |
Causes
If a child is sickly, either with rickets or any other ailment that prevents ossification of the bones, or is improperly fed, the bowed condition may persist. Thus the chief cause of this deformity is rickets. Skeletal problems, infection, and tumors can also affect the growth of the leg, sometimes giving rise to a one-sided bow-leggedness. The remaining causes are occupational, especially among jockeys, and from physical trauma, the condition being very likely to supervene after accidents involving the condyles of the femur.[1]
Childhood
Children until the age of 3 to 4 have a degree of genu varum. The child sits with the soles of the feet facing one another; the tibia and femur are curved outwards; and, if the limbs are extended, although the ankles are in contact, there is a distinct space between the knee-joints. During the first year of life, a gradual change takes place. The knee-joints approach one another; the femur slopes downward and inward towards the knee joints; the tibia become straight; and the sole of the foot faces almost directly downwards.
While these changes are occurring, the bones, which at first consist principally of cartilage, are gradually becoming ossified. By the time a normal child begins to walk, the lower limbs are prepared, both by their general direction and by the rigidity of the bones which form them, to support the weight of the body.[1]
Rickets
Nutritional rickets is an important cause of childhood genu varum or bow legs in some parts of the world. Nutritional rickets is due to unhealthy life style habits as insufficient exposure to sun light which is the main source of vitamin D. Insufficient dietary intake of calcium is another contributing factor. Rickets may also have genetic causes, occasionally called resistant rickets.[2] Rickets usually causes bone deformities in all four extremities. Genu varum may resolve spontaneously with modification of life style activities or after receiving medical treatment. Some deformities do not correct spontaneously and need surgical intervention especially if they are severe and causing gait difficulties. The main surgical modality used to treat genu varum arising from rickets is guided growth surgery, also known as growth modulation surgery. [3]
Blount's disease
Blount's disease is a deformity in the legs, mostly from the knees to the ankles. The affected bone curves in or out and forms the usual "archers bow" which can also be called bow-legs. There are two types of Blount's disease. The first type is Infantile: this means that children under four are diagnosed with this disease. Blount's disease in this age is very risky because sometimes it is not detected and it passes to the second type of Blount's disease. The second type of Blount's disease is found mostly in older children and in teenagers, sometimes in one leg and sometimes in both; the patient's age determines how severe the diagnosis is.[4]
Osteochondrodysplasia
Osteochondrodysplasia are a diverse group of genetic bone diseases or genetic skeletal dysplasias that manifest in generalized bone deformities involving the extremities and the spine. Bow legs or genu varum is one of these deformities. The characteristic bone X-ray survey findings are important to confirm the diagnosis.[5]
Diagnosis
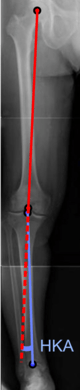
On projectional radiography, the degree of varus or valgus deformity can be quantified by the hip-knee-ankle angle,[6] which is an angle between the femoral mechanical axis and the center of the ankle joint.[7] It is normally between 1.0° and 1.5° of varus in adults.[8] Normal ranges are different in children.[9]
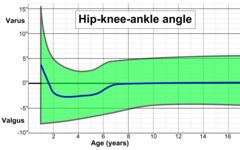 Hip-knee-ankle angle by age, with 95% prediction interval.[9]
Hip-knee-ankle angle by age, with 95% prediction interval.[9]
Treatment
Generally, no treatment is required for idiopathic presentation as it is a normal anatomical variant in young children. Treatment is indicated when it persists beyond 3 and a half years old. In the case of unilateral presentation or progressive worsening of the curvature, when caused by rickets, the most important thing is to treat the constitutional disease, at the same time instructing the care-giver never to place the child on its feet. In many cases this is quite sufficient in itself to effect a cure, but matters can be hastened somewhat by applying splints. When the deformity arises in older patients, either from trauma or occupation, the only permanent treatment is surgery, but orthopaedic bracing can provide relief.
Rickets
Rickets usually causes bone deformities in all four extremities. Genu varum may resolve spontaneously with modification of life style activities or after receiving medical treatment. Some deformities do not correct spontaneously and need surgical intervention especially if they are severe and causing gait difficulties. The main surgical modality used to treat genu varum arising from rickets is guided growth surgery, also known as growth modulation surgery.[3]
Blount's disease
Treatment for children with Blount's disease is typically braces but surgery may also be necessary. In children guided growth surgery is used to gradually correct/straighten the bow legs.[10] For teenagers osteotomy or bone cutting is often used to correct the bone deformity. The operation consists of removing a piece of tibia, breaking the fibula and straightening out the bone; there is also a choice of elongating the legs. If not treated early enough, the condition worsens quickly.[11]
Osteochondrodysplasia
Guided growth surgery in children is widely used to achieve gradual correction of knee deformities arising from Osteochondrodysplasia including genu varum. Yet, this treatment is associated with a high incidence of recurrence and repeated surgeries may be needed to maintain proper bone alignment.[10][5]
Prognosis
In most cases persisting after childhood, there is little or no effect on the ability to walk. Due to uneven stress and wear on the knees, however, even milder manifestations can see an accelerated onset of arthritis.
See also
- Genu valgum
- Genu recurvatum
- Varus deformity
- Rickets
- Knee pain
- Knee osteoarthritis
References
-

- Creo, AL; Thacher, TD; Pettifor, JM; Strand, MA; Fischer, PR (6 December 2016). "Nutritional rickets around the world: an update. Paediatr Int Child Health". Paediatr Int Child Health. 37 (2): 84–98. doi:10.1080/20469047.2016.1248170. PMID 27922335.
- EL-Sobky, TA; Samir, S; Baraka, MM; Fayyad, TA; Mahran, MA; Aly, AS; Amen, J; Mahmoud, S (1 January 2020). "Growth modulation for knee coronal plane deformities in children with nutritional rickets: A prospective series with treatment algorithm". JAAOS: Global Research and Reviews. 4 (1). doi:10.5435/JAAOSGlobal-D-19-00009.
- Shriner's, Hospital for Children – Houston, TX. "Blount's Disease". Archived from the original on November 26, 2011. Retrieved October 28, 2011.
- EL-Sobky, TA; Shawky, RM; Sakr, HM; Elsayed, SM; Elsayed, NS; Ragheb, SG; Gamal, R (15 November 2017). "A systematized approach to radiographic assessment of commonly seen genetic bone diseases in children: A pictorial review". J Musculoskelet Surg Res. 1 (2): 25. doi:10.4103/jmsr.jmsr_28_17.
- W-Dahl, Annette; Toksvig-Larsen, Sören; Roos, Ewa M (2009). "Association between knee alignment and knee pain in patients surgically treated for medial knee osteoarthritis by high tibial osteotomy. A one year follow-up study". BMC Musculoskeletal Disorders. 10 (1): 154. doi:10.1186/1471-2474-10-154. ISSN 1471-2474. PMC 2796991. PMID 19995425.
- Cherian, Jeffrey J.; Kapadia, Bhaveen H.; Banerjee, Samik; Jauregui, Julio J.; Issa, Kimona; Mont, Michael A. (2014). "Mechanical, Anatomical, and Kinematic Axis in TKA: Concepts and Practical Applications". Current Reviews in Musculoskeletal Medicine. 7 (2): 89–95. doi:10.1007/s12178-014-9218-y. ISSN 1935-973X. PMC 4092202. PMID 24671469.
- Sheehy, L.; Felson, D.; Zhang, Y.; Niu, J.; Lam, Y.-M.; Segal, N.; Lynch, J.; Cooke, T.D.V. (2011). "Does measurement of the anatomic axis consistently predict hip-knee-ankle angle (HKA) for knee alignment studies in osteoarthritis? Analysis of long limb radiographs from the multicenter osteoarthritis (MOST) study". Osteoarthritis and Cartilage. 19 (1): 58–64. doi:10.1016/j.joca.2010.09.011. ISSN 1063-4584. PMC 3038654. PMID 20950695.
- Sabharwal, Sanjeev; Zhao, Caixia (2009). "The Hip-Knee-Ankle Angle in Children: Reference Values Based on a Full-Length Standing Radiograph". The Journal of Bone and Joint Surgery, American Volume. 91 (10): 2461–2468. doi:10.2106/JBJS.I.00015. ISSN 0021-9355. PMID 19797583.
- Journeau, P (2020). "Update on guided growth concepts around the knee in children". Orthop Traumatol Surg Res. S1877-0568 (19): S171–S180. doi:10.1016/j.otsr.2019.04.025. PMID 31669550.
- PubMed, Health. "Blount's Disease". Retrieved October 28, 2011.
External links
| Classification | |
|---|---|
| External resources |
- "Bowed Legs". American Academy of Orthopaedic Surgeons.
Reviewed by members of POSNA (Pediatric Orthopaedic Society of North America)