Ankle–brachial pressure index
The ankle-brachial pressure index (ABPI) or ankle-brachial index (ABI) is the ratio of the blood pressure at the ankle to the blood pressure in the upper arm (brachium). Compared to the arm, lower blood pressure in the leg suggests blocked arteries due to peripheral artery disease (PAD). The ABPI is calculated by dividing the systolic blood pressure at the ankle by the systolic blood pressure in the arm.[1]
| Ankle–brachial pressure index | |
|---|---|
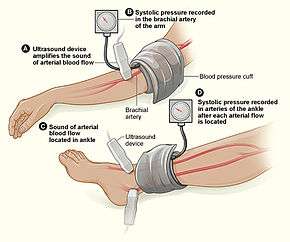 Measuring the ankle-brachial index | |
| Synonyms | Ankle-brachial index |
| Purpose | Detection of peripheral artery disease |
Method
The patient must be placed supine, without the head or any extremities dangling over the edge of the table. Measurement of ankle blood pressures in a seated position will grossly overestimate the ABI (by approximately 0.3).
A Doppler ultrasound blood flow detector, commonly called Doppler wand or Doppler probe, and a sphygmomanometer (blood pressure cuff) are usually needed. The blood pressure cuff is inflated proximal to the artery in question. Measured by the Doppler wand, the inflation continues until the pulse in the artery ceases. The blood pressure cuff is then slowly deflated. When the artery's pulse is re-detected through the Doppler probe the pressure in the cuff at that moment indicates the systolic pressure of that artery.
The higher systolic reading of the left and right arm brachial artery is generally used in the assessment. The pressures in each foot's posterior tibial artery and dorsalis pedis artery are measured with the higher of the two values used as the ABI for that leg.[2]
-
- Where PLeg is the systolic blood pressure of dorsalis pedis or posterior tibial arteries
- and PArm is the highest of the left and right arm brachial systolic blood pressure

The ABPI test is a popular tool for the non-invasive assessment of Peripheral vascular disease (PVD). Studies have shown the sensitivity of ABPI is 90% with a corresponding 98% specificity for detecting hemodynamically significant (Serious) stenosis >50% in major leg arteries, defined by angiogram.[3]
However, ABPI has known issues:
- ABPI is known to be unreliable on patients with arterial calcification (hardening of the arteries) which results in less or incompressible arteries,[4] as the stiff arteries produce falsely elevated ankle pressure, giving false negatives[5]). This is often found in patients with diabetes mellitus[6] (41% of patients with peripheral arterial disease (PAD) have diabetes[7]), kidney failure or heavy smokers. ABPI values below 0.9 or above 1.3 should be investigated further regardless.
- Resting ABPI is insensitive to mild PAD.[8] Treadmill tests (6 minute) are sometimes used to increase ABPI sensitivity,[9] but this is unsuitable for patients who are obese or have co-morbidities such as Aortic aneurysm, and increases assessment duration.
- Lack of protocol standardisation,[10] which reduces intra-observer reliability.[11]
- Skilled operators are required for consistent, accurate results.[12]
When performed in an accredited diagnostic laboratory, the ABI is a fast, accurate, and painless exam, however these issues have rendered ABI unpopular in primary care offices and symptomatic patients are often referred to specialty clinics[13] due to the perceived difficulties. Technology is emerging that allows for the oscillometric calculation of ABI, in which simultaneous readings of blood pressure at the levels of the ankle and upper arm are taken using specially calibrated oscillometric machines.
Interpretation of results
In a normal subject the pressure at the ankle is slightly higher than at the elbow (there is reflection of the pulse pressure from the vascular bed of the feet, whereas at the elbow the artery continues on some distance to the wrist).
The ABPI is the ratio of the highest ankle to brachial artery pressure. An ABPI between and including 0.90 and 1.29 considered normal (free from significant PAD), while a lesser than 0.9 indicates arterial disease.[14] An ABPI value of 1.3 or greater is also considered abnormal, and suggests calcification of the walls of the arteries and incompressible vessels, reflecting severe peripheral vascular disease.
Provided that there are no other significant conditions affecting the arteries of the leg, the following ABPI ratios can be used to predict the severity of PAD as well as assess the nature and best management of various types of leg ulcers:[2]
| ABPI value | Interpretation | Action | Nature of ulcers, if present |
|---|---|---|---|
| 1.3 and above | Abnormal Vessel hardening from PVD | Refer or measure Toe pressure | Venous ulcer use full compression bandaging |
| 1.0 - 1.2 | Normal range | None | |
| 0.90 - 0.99 | Acceptable | ||
| 0.80 - 0.89 | Some arterial disease | Manage risk factors | |
| 0.50 - 0.79 | Moderate arterial disease | Routine specialist referral | Mixed ulcers use reduced compression bandaging |
| under 0.50 | Severe arterial disease | Urgent specialist referral | Arterial ulcer no compression bandaging used |
Predictor of atherosclerosis mortality
Studies in 2006 suggests that an abnormal ABPI may be an independent predictor of mortality, as it reflects the burden of atherosclerosis.[15][16] It thus has potential for screening for coronary artery disease,[17] although no evidence-based recommendations can be made about screening in low-risk patients because clinical trials are lacking.[17]
References
- Al-Qaisi, M; Nott, DM; King, DH; Kaddoura, S (2009). "Ankle brachial pressure index (ABPI): An update for practitioners". Vascular Health and Risk Management. 5: 833–41. doi:10.2147/vhrm.s6759. PMC 2762432. PMID 19851521.
- Vowden P, Vowden K (March 2001). "Doppler assessment and ABPI: Interpretation in the management of leg ulceration". Worldwide Wounds. - describes ABPI procedure, interpretation of results, and notes the somewhat arbitrary selection of "ABPI of 0.8 has become the accepted endpoint for high compression therapy, the trigger for referral for a vascular surgical opinion and the defining upper marker for an ulcer of mixed aetiology"
- McDermott MM, Criqui MH, Liu K, Guralnik JM, Greenland P, Martin GJ, Pearce W (December 2000). "Lower ankle/brachial index, as calculated by averaging the dorsalis pedis and posterior tibial arterial pressures, and association with leg functioning in peripheral arterial disease". J Vasc Surg. 32 (6): 1164–71. doi:10.1067/mva.2000.108640. PMID 11107089.
- Allison MA, Hiatt WR, Hirsch AT, Coll JR, Criqui MH (April 2008). "A high ankle-brachial index is associated with increased cardiovascular disease morbidity and lower quality of life". J Am Coll Cardiol. 51 (13): 1292–8. doi:10.1016/j.jacc.2007.11.064. PMID 18371562.
- American Diabetes Association (December 2003). "Peripheral Arterial Disease in People with Diabetes". Diabetes Care. 26 (12): 3333–3341. doi:10.2337/diacare.26.12.3333. PMID 14633825.
- Aboyans V, Ho E, Denenberg JO, Ho LA, Natarajan L, Criqui MH (November 2008). "The association between elevated ankle systolic pressures and peripheral occlusive arterial disease in diabetic and nondiabetic subjects". J Vasc Surg. 48 (5): 1197–203. doi:10.1016/j.jvs.2008.06.005. PMID 18692981.
- Novo S (March 2002). "Classification, epidemiology, risk factors, and natural history of peripheral arterial disease". Diabetes Obes Metab. 4: S1–6. doi:10.1046/j.1463-1326.2002.0040s20s1.x. PMID 12180352.
- Stein R, Hriljac I, Halperin JL, Gustavson SM, Teodorescu V, Olin JW (February 2006). "Limitation of the resting ankle-brachial index in symptomatic patients with peripheral arterial disease" (PDF). Vasc Med. 11 (1): 29–33. doi:10.1191/1358863x06vm663oa. PMID 16669410.
- Montgomery PS, Gardner AW (June 1998). "The clinical utility of a six-minute walk test in peripheral arterial occlusive disease patients". J Am Geriatr Soc. 46 (6): 706–11. doi:10.1111/j.1532-5415.1998.tb03804.x. PMID 9625185.
- Jeelani NU, Braithwaite BD, Tomlin C, MacSweeney ST (July 2000). "Variation of method for measurement of brachial artery pressure significantly affects ankle-brachial pressure index values". Eur J Vasc Endovasc Surg. 20 (1): 25–8. doi:10.1053/ejvs.2000.1141. PMID 10906293.
- Caruana MF, Bradbury AW, Adam DJ (May 2005). "The validity, reliability, reproducibility and extended utility of ankle to brachial pressure index in current vascular surgical practice". Eur J Vasc Endovasc Surg. 29 (5): 443–51. doi:10.1016/j.ejvs.2005.01.015. PMID 15966081.
- Kaiser V, Kester AD, Stoffers HE, Kitslaar PJ, Knottnerus JA (July 1999). "The influence of experience on the reproducibility of the ankle-brachial systolic pressure ratio in peripheral arterial occlusive disease". Eur J Vasc Endovasc Surg. 18 (1): 25–9. doi:10.1053/ejvs.1999.0843. PMID 10388635.
- Hirsch AT, Criqui MH, Treat-Jacobson D, Regensteiner JG, Creager MA, Olin JW, Krook SH, Hunninghake DB, Comerota AJ, Walsh ME, McDermott MM, Hiatt WR (Sep 2001). "Peripheral arterial disease detection, awareness, and treatment in primary care". JAMA. 286 (11): 1317–24. doi:10.1001/jama.286.11.1317. PMID 11560536.
- Rooke, TW; Hirsch, AT; Misra, S; Sidawy, AN; Beckman, JA; Findeiss, LK; Golzarian, J; Gornik, HL; Halperin, JL; Jaff, MR; Moneta, GL; Olin, JW; Stanley, JC; White, CJ; White, JV; Zierler, RE; Society for Cardiovascular Angiography and, Interventions; Society of Interventional, Radiology; Society for Vascular, Medicine; Society for Vascular, Surgery (Nov 1, 2011). "2011 ACCF/AHA Focused Update of the Guideline for the Management of Patients With Peripheral Artery Disease (updating the 2005 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines". Journal of the American College of Cardiology. 58 (19): 2020–45. doi:10.1016/j.jacc.2011.08.023. PMC 4714326. PMID 21963765.
- Feringa HH, Bax JJ, van Waning VH, et al. (March 2006). "The long-term prognostic value of the resting and postexercise ankle-brachial index". Arch. Intern. Med. 166 (5): 529–35. doi:10.1001/archinte.166.5.529. PMID 16534039.
- Wild SH, Byrne CD, Smith FB, Lee AJ, Fowkes FG (March 2006). "Low ankle-brachial pressure index predicts increased risk of cardiovascular disease independent of the metabolic syndrome and conventional cardiovascular risk factors in the Edinburgh Artery Study". Diabetes Care. 29 (3): 637–42. doi:10.2337/diacare.29.03.06.dc05-1637. PMID 16505519.
- Desai, Chintan S.; Blumenthal, Roger S.; Greenland, Philip (2014). "Screening low-risk individuals for coronary artery disease". Current Atherosclerosis Reports. 16 (4): 402. doi:10.1007/s11883-014-0402-8. ISSN 1534-6242. PMID 24522859.
External links
- medical test information form (PDF) at webMD
- Ankle Brachial Index at Stanford Medicine 25