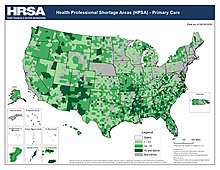
Medical deserts in the United States
The United States has many regions which have been described as medical deserts, regions with inadequate access to one or more kinds of medical services. An estimated 30 million Americans, many in rural regions of the country, live at least 60 minutes drive from a hospital with trauma care services.[1] Limited access to emergency room services, as well as medical specialists, leads to increases in mortality rates and long-term health problems, such as heart disease and diabetes.[2][3] Regions with higher rates of Medicaid and Medicare patients, as well patients who are uninsured are less likely to live within an hour's drive of a hospital emergency room.[1]
Since 1975, over 1,000 hospitals, many in rural regions, have closed their doors, unable to bear the cost of care of uninsured patients,[4] resulting in some patients in every state needing to drive at least an hour to a hospital emergency room, a problem that poses an even greater danger during the COVID-19 pandemic, when patients in respiratory distress urgently need oxygen[5] and can ill afford an hour-long ambulance ride to reach a hospital. In addition to the immediate financial problems facing rural healthcare providers, inequities in rural healthcare are further aggravated by the disproportionately low amount of newly graduated doctors that apply for positions in rural areas.
Although concentrated in rural regions, health care deserts also exist in urban and suburban areas, particularly in Black majority census tracts[6] in Chicago, Los Angeles and New York City. Medical literature addressing health disparities in urban centers has applied the term medical desert to areas that are more than a five-miles from the nearest acute care facility.[6] Racial demographic disparities in healthcare access are also present in rural areas, with Native Americans living in rural areas in particular receiving inadequate medical care.[7][8]

Proposed solutions to US health care deserts include the enactment of a national single payer health care system; adoption of a public option under the Affordable Care Act (ACA); the approval of higher Medicare reimbursements and tax credits for struggling hospitals; the establishment of strategically placed free-standing emergency centers; the expansion of telehealth and telemedicine to remote areas; and increased incentives to recruit doctors to practice in rural and underserved areas.
Rural health care deserts
In 2019, the federal government identified nearly 80 percent of rural America as “medically underserved,”[9] lacking in skilled nursing facilities, as well as rehabilitation, psychiatric and intensive care units.[10] In rural areas, there are approximately 68 primary care doctors per 100,000 people, whereas there are 84 doctors per 100,000 in urban centers.[11] According to the National Rural Health Association, 9% of rural counties had no doctors in 2017. Rural communities face lower life expectancy and increased rates of diabetes, chronic disease, and obesity.[12] Fewer than half of rural women live within a thirty-minute drive of the nearest hospital able to provide obstetric services, and 12% do not live within a sixty-minute drive of the nearest such hospital, resulting in babies sometimes being born on the side of the road and increased maternal and infant mortality rates.[13]
Rural residents may live on farms, ranches and Indian reservations far from a hospital, forcing residents to take several hours or an entire day off work to drive to a doctor's appointment or follow up care, making rural residents less likely to seek treatment.[14] The Centers for Disease Control and Prevention (CDC) reports that during 1999–2014 rural counties experienced increased mortality rates from the five leading causes of death (1-heart disease, 2-cancer, 3-unintentional injury, 4-chronic lower respiratory disease (CLRD), 5-stroke) compared with metropolitan counties. For unintentional injuries (high speed car accidents; opioid and drug abuse and traumatic brain injuries) mortality rates were approximately 50% higher in rural areas than urban areas", with inadequate access to adequately staffed healthcare facilities listed as one among several factors leading to this disparity.[15]
In states that chose not to expand Medicaid programs under the Affordable Care Act–Alabama, Georgia, Missouri, Oklahoma, Texas and Tennessee–rural Americans face limited options as hospitals close their doors. A 2019 study found that participation in Medicaid expansion reduced the likelihood of rural hospital closures by 62% and that of the hospitals deemed most at-risk for closure, 75% were in states that did not expand Medicare.[16]
In 2016, the Kaiser Commission on Medicaid and the Uninsured, in conjunction with the Urban Institute, conducted a case study analysis of three privately owned Southern hospitals to determine the causes and effects of their closures in Kansas, Kentucky and South Carolina. In addition to the challenges of graying, declining and poverty-stricken populations, as well as the preference of privately insured patients to seek treatment at newer hospitals further away, the report said corporate profit-driven decisions, as opposed to local community needs, shuttered the doors of rural hospitals in underserved areas. In a "shift from mission to margin," health systems that owned multiple hospitals, some more profitable than others, closed less-profitable hospitals in Kentucky and South Carolina to concentrate resources on other hospitals in the chain, resulting in communities without acute care and emergency facilities to serve as a safety-net for patients facing challenges with mental health and drug use. The case studies report also notes that decreases in Medicare and Medicaid reimbursements, some the result of federal budget sequestration or across the board cuts, others the result of the Affordable Care Act's lower hospital Medicare readmission reimbursement rates, negatively impacted the finances of the rural hospitals.[17]
Physician shortages
About 20% of Americans live in rural regions, but only nine percent of the country's doctors practice in rural areas.[18] Federal health officials predicted in 2019 that the number of rural doctors, half of them over 50 years of age, would decline by 23 percent during the next ten years.[9] A contributing factor to this decline is newly graduated doctors' reluctance to move to rural areas. While doctors originally from rural areas are more likely to return to rural areas to practice, rural Americans are less likely to attend medical school in the first place.[11] Newly graduated doctors have also tended to prefer jobs in hospitals, rather than jobs in family practices that are more common in rural areas.[19]
Only 1% of medical students in their final year of school prefer to live in communities under 10,000. The lack of entertainment or food diversity, fear of prejudice, and reduced financial prospects associated with rural regions are have been cited as factors leading to medical students' reluctance to practice in rural regions, as well as the unique difficulties associated with practice rural healthcare.[11] For example, in parts of rural Alaska, transferring patients to hospital emergency rooms can "depend on the schedules of rickety charter planes" which are often prevented from flying due to the weather.[11] In some states, such as Oklahoma, a lack of available residency programs for prospective doctors directly contributes to a shortage.[20]

Impact on Native Americans and Alaskan Natives


The federal government is legally obligated under treaties to provide medical care to American Indian and Alaska Native Americans through the Indian Health Service (IHS), part of the United States Department of Health and Human Services.[21] Advocates for the Native American community have argued, however, that the government chronically under funds the IHS, resulting in a lack of accessible health care facilities, particularly emergency room departments for those living on reservations.[22] The IHS provides services to 573 tribes and 2.56 million Native Americans primarily living on or near reservations and in rural areas concentrated in Alaska and the western United States. In 2011, the IHS reported that life expectancy for Native Americans was 73, compared to 78 for all other races in the US, as Native Americans and Alaskan natives were dying at higher rates due to chronic liver disease, diabetes, intentional self-harm and suicide, as well as respiratory diseases.[23] In 2016, the Office of Inspector General (OIG) issued reports criticizing the IHS's hospital care for tribal members, citing lack of oversight, outdated equipment and difficulty in recruiting and retaining skilled staff. Administrators at one hospital interviewed by the OIG complained of aging hospital infrastructure with corroded pipes causing sewage to spill into an operating room.[24]
Dissatisfied with the IHS's management of health clinics and hospitals closest to reservations, tribes have demanded greater control over hospital administration. In July, 2019, the Great Plains Tribal Chairmen's Health Board representing 18 tribal communities in South Dakota, North Dakota, Nebraska and Iowa, took over the Rapid City's Sioux San Hospital, where, according to government investigators, patients died as a result of misdiagnoses and treatment by staff members not screened for hepatitis and tuberculosis.[25]
In New Mexico, where Native Americans, in 2020, make up six percent of the population but 25% of positive COVID-19 cases, members of the Navajo Nation live without access to running water to frequently wash their hands, as recommended by the CDC.[26][27]
Urban health care deserts
.jpg)
According to research conducted in 2019 by University of Chicago Medicine, African American census tracts in large US cities—Chicago, Los Angeles, New York City—are more likely than white majority neighborhoods to be located in trauma care deserts that are greater than five miles from a trauma center offering emergency medical services and specialists: neurosurgeons, cardiac doctors, respiratory therapists.[28]

A team of researchers found that in Los Angeles 89 percent of Black-majority census tracts were situated in trauma deserts; in Chicago, 73 percent; in New York City 14 percent.[6] In Los Angeles County, South Los Angeles with one-million residents and the highest mortality rate in the county, also has the highest rates of disease and premature deaths from preventable conditions: "coronary heart disease, homicide, diabetes, lung cancer, and motor vehicle crashes."[29] In economically stressed South LA, there are 11 pediatricians for every 100,000 children, whereas in upscale West Los Angeles there are almost 200 pediatricians for every100,000 children. In West LA, 12 percent of adults are uninsured compared to 30 percent in South LA.[30]
Even as health care delivery models shift from hospitals to community clinics offering Urgent Care in once-vacant retail spaces, poor neighborhoods face inequities with the distribution of community clinics in predominantly wealthier suburban neighborhoods.[31]
COVID-19 impacts on urban communities of color
African Americans account for a disproportionate number of COVID-19 fatalities due to multiple factors, including greater exposure in use of public transportation and employment in care-giving, sanitation and retail, underlying health conditions, as well as lack of access to nearby medical health clinics and hospitals and inadequate health insurance.[32] In an April 2020 analysis of early data, the Washington Post found that counties with a majority of Black residents faced three times the rate of COVID-19 infections and almost six times the rate of deaths as majority white counties.[33] The American Medical Association (AMA), noting structural inequities gripping communities of color, urged the federal government to collect COVID-19 data by race and ethnicity.[34]
During the COVID-19 crisis, New York Times reporter Michael Schwirtz wrote (April 26, 2020) of the disparities in hospital services and finances between New York's white communities and those of color, with a private hospital closer to Wall Street able to tap reserves and exercise political influence to treat more patients, boost testing and obtain protective gear, even arrange for a plane from billionaire Warren Buffett's company to fly in masks from China, while a Brooklyn public hospital serving patients predominantly poor and of color resorts to plastic and duct tape to separate infectious patients' quarters and launches a Go Fund Me page to raise money for masks, gowns and booties to protect doctors and nurses from a virus that is "killing black and Latino New Yorkers at about twice the rate of white residents."[35]
Racial disparities in health care
Scholars and researchers trace the roots of African American health care inequities to chattel slavery, Jim Crow laws and institutional racism, with medical schools perpetuating stereotypes of racial inferiority up until the mid 20th century and scientists exploiting African Americans in unethical experimentation without informed consent.[36] In The Atlantic's "Why American Health Care is still Segregated" (2016), reporter Vann Newkirk writes of Black Codes[37] that led to racially segregated clinics, doctors' offices and hospitals in which African Americans were assigned to separate wings to receive inferior medical treatment.[38] In a 2008 address to the National Medical Association in 2008, Ronald M. Davis, MD, past president of the American Medical Association (AMA), apologized for the organization's history of excluding African-Americans from the AMA, pledging to "right the wrongs perpetrated against African American physicians, their families and patients."[39]
Hundreds of years of geographical segregation left a legacy of segregated and understaffed hospitals serving African American communities.[40] In a departure from the past, the National Association for the Advancement of Colored People (NAACP) in the 1960s won a US Supreme Court victory in Simkins v Moses H. Cone Memorial Hospital, a landmark ruling that barred the use of public funds to expand segregated hospitals.[41] Still, racial segregation in the medical field persists, with African Americans living in Black neighborhoods more likely than whites to undergo treatment at hospitals with higher surgical death rates, give birth at hospitals with higher neonatal mortality rates and live in nursing homes with fewer staff members and tenuous finances.[42]
The 2010 passage of the Affordable Care Act expanded Medicaid eligibility for low income Americans, but several Southern states with large poor Black populations opted out of the expansion, its Republican governors opposing the Obama-led initiative as federal over-reach.[38] In rejecting Medicaid expansion—estimated at $100 billion federal dollars over 10 years—then Texas Governor Rick Perry told Tea Party supporters in 2013, "Texas will not be held hostage by the Obama administration's attempt to force us into this fool's errand of adding more than a million Texans to a broken system."[43]
Suburban health care deserts
Though suburbs often conjure images of affluence, a Health Affairs study using national survey data from 2005 to 2015 belies that picture. According to the survey, the suburbs, receiving a fraction of public health care funding compared to cities, are home to 17 million Americans who struggle in poverty, exceeding the numbers in urban centers and rural areas and straining hospitals with aging infrastructure. Additionally, the Health Affairs study noted large numbers of uninsured or Medicaid-reliant suburban dwellers either can't find doctors and hospitals who will serve them or must travel great distances to see specialists.[44][45]
Proposed solutions
Single-payer health care / Medicare for All
.jpg)
Proponents of a national health insurance program to replace for-profit health insurance argue adoption of a federally funded single-payer system allowing patients to choose their own doctor would reduce "structural racism" in health care that results in non-white Americans suffering higher mortality rates in underserved communities. Backers of single-payer or Medicare for All note that minorities and the poor, as well as rural residents,[46] in general, are less able to afford private health insurance, and that those who can must pay high deductibles and co-payments that threaten families with financial ruin.[47] In addition, they argue that those with employment-based insurance are tethered to jobs for fear of losing their medical coverage while rural communities with high unemployment lose out on job-based insurance benefits.[48]
Critics of Medicare for All oppose a government funded health care system, wanting to preserve a for-profit model to increase competition, and assert that hospitals, already financially vulnerable in rural America, would lose more money and risk bankruptcy because private insurance, on which they rely for financial stability, reimburses at higher rates than Medicare.[49] Proponents argue, however, that proposed single-payer legislation in the House[50] and Senate[51] would boost hospital reimbursements far beyond current levels, while establishing annual global hospital funds that could be increased to cover unexpected costs and grant applications for capital improvements .[52] Supporters of single-payer point to the closure of over 100 rural hospitals since 2010, with over 400 also at risk of closure, as evidence of the failure of a for-profit health insurance system unaffordable to many rural residents and unsustainable for hospitals that rely on reimbursements from private insurance.[53]
Public option to the Affordable Care Act (ACA)
.jpg)
Proponents of a public option support expanding the Affordable Care Act to give consumers a choice; private for-profit health insurance or Medicare. Backers of the public option say the ACA has not gone far enough, noting that despite the United States spending a greater percentage of its GDP on health care than any other nation, there are still over 28-million people without health insurance, resulting in Americans in underserved communities dying for lack of affordable care or declaring bankruptcy because of mounting medical bills.[54]
While advocates of a public option agree with single-payer proponents that the United States should provide universal health care, they disagree on the solution, asserting that Americans are not interested in a government-run health care system and want to be able to keep their private health insurance.[55] Critics who support single-payer instead charge that offering a public option to compete with private insurance would create a two-tiered system of concierge versus minimal medical services, as private for-profit insurance companies use political muscle to deny coverage to the oldest and sickest Americans, thus shunting the more expensive patients onto a financially vulnerable public option.[56] Medicare for All proponents also say a hybrid system of private insurance coupled with a public option would result in added bureaucracy and paperwork, and therefore fail to lower health care costs.[57]
Those favoring a strictly for-profit health care model claim a public option, with lower hospital reimbursements than private insurance, would bankrupt rural hospitals dependent on higher reimbursements from commercial insurance vendors.[58]
Higher medical reimbursements and tax credits for rural hospitals
Seema Verma, Administrator of the Centers for Medicare & Medicaid Services (CMS), explains wage index disparities between urban and rural hospitals that led to underfunding rural hospitals will no longer strictly determine Medicare and Medicaid reimbursements.[59] Under new policy rules, struggling rural hospitals may be eligible for higher Medicare reimbursements which, according to CMS, can be used to attract more highly skilled medical professionals.[60] In addition, CMS will expand rural telehealth services under Medicare Advantage, a privatized insurance program, and relax supervision requirements for physician assistants and radiologist assistants.[59]
On the state level, in 2016 Georgia established a $60 billion tax credit program to allow hospital donors to write off 100% of their donation to support a rural hospital. An investigation by the state's Department of Audits and Accounts found, however, the donations were not benefiting the rural hospitals that need the funds the most because too much money was deposited in the bank accounts of third party partners.[61] Lawmakers have also complained that tax credits have benefited at least one rural hospital with a $60 million profit margin.[62]
Free standing emergency centers (FECs)
In light of large numbers of hospital closures, particularly in rural America where the lack of emergency room services spawn health care deserts, proponents of 24-hour free standing emergency centers (FECs) advocate for more FECs that, unlike Urgent Care centers, would expand offerings beyond primary care to include:[63]
- Advanced laboratory equipment (x-rays; CT scans)
- Emergency trained doctors and nurses
- Pre-arranged transfer for patients requiring hospitalization
- Prolonged 24-hour observation care
FECs can function as outpatient departments for existing hospitals or as independently owned entities. One obstacle to the establishment of additional independently run FECs is the inability to receive Medicare and Medicaid reimbursements afforded only to licensed hospitals. Some FECs have overcome this barrier by establishing licensed micro-hospitals with eight to ten inpatient beds in underserved regions. Another obstacle to growth of FECs in underserved areas is the preference of for-profit health systems to place FECs in dense urban communities that will attract more patients and generate more money while replacing hospital-based emergency services and primary care. Advocates of the FEC model for hard-pressed communities argue the federal government should expand the recognition of independent FECs as Medicare and Medicaid participants in underserved areas.[64]
Telehealth
To address the rural health care crisis, advocates of telehealth promote the use of digital information and communication technology—cell phones and computers—that can be accessed from home or work without encumbering the patient with long travel times to hospitals at least 60 miles from their residence. Proponents say telehealth or remote medical attention can provide patients in health care deserts with greater access to specialists unavailable in rural communities while encouraging patients to assume a greater role in managing their own health care and improving communication between them and their team of doctors. For example, with telehealth a diabetic patient might:[65]
- Video conference with a doctor or other medical professional
- Download an app to estimate, based on diet and activity, the amount of insulin needed.
- Use a cell phone to upload food diaries and blood sugar levels for review by medical professionals
- Watch a video on carbohydrate counting to better control glucose levels
- Access an on-line patient portal to view test results, request pharmacy prescriptions, email a doctor or schedule an appointment
- Receive email reminders to obtain a flu shot or other preventative care
The Heritage Foundation, a think tank advocating limited government, advocates for removal of federal obstacles in order to classify telehealth as preventative care under high deductible insurance plans, provide reimbursements for telehealth visits equal to in-person doctor visits and permit doctors licensed in one state to practice telemedicine across state lines.[66]
Critics of telehealth argue on-line doctor visits are no substitute for in-person evaluations which can provide a more accurate diagnosis and that uninsured rural Americans still won't be able to afford quality medical care. In addition, they argue large swaths of rural America may not have access to broadband internet[67] necessary for successful implementation of telehealth.
Incentives to recruit skilled medical professionals
The federal Office of Rural Health Policy oversees the non-profit National Rural Recruitment and Retention Network to connect medical professionals, hospitals and clinics in rural areas with recruitment and retention resources. The Network lists the following incentives rural legislative and medical entities could offer prospective doctors: health insurance, retirement packages, sabbaticals, sign-on bonuses, low-interest home loans.[68] The Indian Health Service (IHS) offers prospective doctors up to $40,000 for repayment of student loans in exchange for a two-year commitment to serve American Indian and Alaska Native communities. Similarly, the National Health Service Corps (NHSC) offers up to $50,000 toward loan repayment if licensed health care providers agree to practice for two years in an underserved area. Under the federal NIMHD Loan Repayment Program (LRP) health professionals with doctoral degrees can receive up to $50,000 per year for two years to conduct research on health disparities.[69]
References
- Carr, Brendan; Bowman, Ariel; Wolff, Catherine; Mullen, Michael T.; Holena, Daniel; Branas, Charles C.; Wiebe, Douglas (2017). "Disparities in Access to Trauma Care in the United States: A Population-Based Analysis". Injury. 48 (2): 332–338. doi:10.1016/j.injury.2017.01.008. ISSN 0020-1383. PMC 5292279. PMID 28069138.
- "Poor Access to a Trauma Center Linked to Higher Prehospital Death Rates in More Than Half of U.S. States". American College of Surgeons. Retrieved 2020-04-24.
- "About Rural Health Care - NRHA". www.ruralhealthweb.org. Retrieved 2020-04-24.
- "Hospital Closings Likely to Increase". Official web site of the U.S. Health Resources & Services Administration. 2017-10-16. Retrieved 2020-04-25.
- "Neighborhoods With 'Medical Deserts' Have Emergency Needs During COVID Pandemic". The Baltimore Times, Inc. Positive Stories. Retrieved 2020-04-24.
- Tung, Elizabeth L.; Hampton, David A.; Kolak, Marynia; Rogers, Selwyn O.; Yang, Joyce P.; Peek, Monica E. (2019-03-01). "Race/Ethnicity and Geographic Access to Urban Trauma Care". JAMA Network Open. 2 (3): e190138. doi:10.1001/jamanetworkopen.2019.0138. PMID 30848804.
- "For Native Americans, Health Care Is A Long, Hard Road Away". NPR.org. Retrieved 2020-04-24.
- Press, The Associated (2016-10-08). "Why Care at Native American Hospitals Is Often Substandard". The New York Times. ISSN 0362-4331. Retrieved 2020-04-24.
- Saslow, Eli (2019). "'Out here, it's just me': In the medical desert of rural America, one doctor for 11,000 square miles". Washington Post.
- "National Healthcare Quality and Disparities Report" (PDF). U.S. Department of Health and Human Services. 2017.
- Khazan, Olga (2014-08-28). "Would You Want to Move to a Remote Alaskan Village?". The Atlantic. Retrieved 2020-04-24.
- "Medical deserts in America: Why we need to advocate for rural healthcare". globalhealth.harvard.edu. Retrieved 2020-04-24.
- Maron, Dina Fine. "Maternal Health Care Is Disappearing in Rural America". Scientific American. Retrieved 2020-04-27.
- "Health Disparities Affect Millions in Rural U.S. Communities". AAMC. Retrieved 2020-04-24.
- Garcia, Macarena C. (2017). "Reducing Potentially Excess Deaths from the Five Leading Causes of Death in the Rural United States". MMWR. Surveillance Summaries. 66 (2): 1–7. doi:10.15585/mmwr.ss6602a1. ISSN 1546-0738. PMC 5829929. PMID 28081057.
- Scott, Dylan (2020-02-18). "1 in 4 rural hospitals is vulnerable to closure, a new report finds". Vox. Retrieved 2020-04-25.
- Wishner, Jane; Solleveld, Patricia; Paradise, Julia; Jul 07, Larisa Antonisse Published:; 2016 (2016-07-07). "A Look at Rural Hospital Closures and Implications for Access to Care: Three Case Studies - Issue Brief". The Henry J. Kaiser Family Foundation. Retrieved 2020-04-27.CS1 maint: extra punctuation (link) CS1 maint: numeric names: authors list (link)
- Rosenblatt, Roger A; Hart, L Gary (2000). "Physicians and rural America". Western Journal of Medicine. 173 (5): 348–351. doi:10.1136/ewjm.173.5.348. ISSN 0093-0415. PMC 1071163. PMID 11069878.
- "The Struggle To Hire And Keep Doctors In Rural Areas Means Patients Go Without Care". NPR.org. Retrieved 2020-04-24.
- "Oklahoma is a physician 'desert,' state medical leader says". www.beckershospitalreview.com. Retrieved 2020-04-24.
- "Basis for Health Services | Fact Sheets". Newsroom. 2013-01-01. Retrieved 2020-04-27.
- "For Native Americans, Health Care Is A Long, Hard Road Away". NPR.org. Retrieved 2020-04-24.
- "Disparities | Fact Sheets". Newsroom. 2013-01-01. Retrieved 2020-04-24.
- Press, The Associated (2016-10-08). "Why Care at Native American Hospitals Is Often Substandard". The New York Times. ISSN 0362-4331. Retrieved 2020-04-24.
- Walker, Mark (2019-10-15). "Fed Up With Deaths, Native Americans Want to Run Their Own Health Care". The New York Times. ISSN 0362-4331. Retrieved 2020-04-24.
- Beavers, David. "Mayors, governor call out racial health disparities highlighted by coronavirus". POLITICO. Retrieved 2020-04-27.
- "Indian Country faces higher risks, lack of resources in COVID-19 fight". ABC News. Retrieved 2020-04-27.
- "Study: Urban African-Americans more likely to live in trauma deserts". www.uchicagomedicine.org. Retrieved 2020-04-24.
- Park, Watson, Galloway-Gilliam (2008). "South Los Angeles Health Equity Scorecard" (PDF).CS1 maint: multiple names: authors list (link)
- Park, Watson, Gilliam (2008). "South Los Angeles Health Equity Scorecard" (PDF).CS1 maint: multiple names: authors list (link)
- "Healthcare Deserts Being Left Behind As Systems Expand Care Into Communities". Bisnow. Retrieved 2020-04-25.
- "Why African-Americans may be especially vulnerable to COVID-19". Science News. 2020-04-10. Retrieved 2020-04-25.
- Scott, Eugene (2020). "4 reasons coronavirus is hitting black communities so hard". Washington Post.
- Cooney, Elizabeth (April 9, 2020). "Who gets hospitalized for Covid-19? Report shows differences by race and sex". Statenews.com.
- Schwirtz, Michael; Luce, Kirsten (2020-04-26). "One Rich N.Y. Hospital Got Warren Buffett's Help. This One Got Duct Tape". The New York Times. ISSN 0362-4331. Retrieved 2020-04-26.
- Byrd, W. M.; Clayton, L. A. (March 2001). "Race, medicine, and health care in the United States: a historical survey". Journal of the National Medical Association. 93 (3 Suppl): 11S–34S. ISSN 0027-9684. PMC 2593958. PMID 12653395.
- "Black Codes (United States)", Wikipedia, 2020-04-22, retrieved 2020-04-27
- II, Vann R. Newkirk (2016-05-18). "Why American Health Care Is Still Segregated". The Atlantic. Retrieved 2020-04-27.
- "The history of African Americans and organized medicine". American Medical Association. Retrieved 2020-04-24.
- II, Vann R. Newkirk (2016-05-18). "Why American Health Care Is Still Segregated". The Atlantic. Retrieved 2020-04-24.
- Reynolds, P. P. (1997-06-01). "Hospitals and Civil Rights, 1945-1963: the case of Simkins v Moses H. Cone Memorial Hospital". Annals of Internal Medicine. 126 (11): 898–906. doi:10.7326/0003-4819-126-11-199706010-00009. ISSN 0003-4819. PMID 9163292.
- Smith, David Barton; Feng, Zhanlian; Fennell, Mary L.; Zinn, Jacqueline S.; Mor, Vincent (2007-09-01). "Separate And Unequal: Racial Segregation And Disparities In Quality Across U.S. Nursing Homes". Health Affairs. 26 (5): 1448–1458. doi:10.1377/hlthaff.26.5.1448. ISSN 0278-2715. PMID 17848457.
- "Texas Politicians And Businesses Feud Over Medicaid Expansion". NPR.org. Retrieved 2020-04-27.
- Schnake-Mahl, Alina S.; Sommers, Benjamin D. (2017-10-01). "Health Care In The Suburbs: An Analysis Of Suburban Poverty And Health Care Access". Health Affairs. 36 (10): 1777–1785. doi:10.1377/hlthaff.2017.0545. ISSN 0278-2715. PMID 28971923.
- Healthline, Elaine Korry, California (2018-01-31). "Growing number of suburban poor discover health care's nowhere land". CNNMoney. Retrieved 2020-04-25.
- "Health Care In Rural America". Center for Rural Affairs. 2007-08-22. Retrieved 2020-04-25.
- "Single-Payer Health Reform: A Step Toward Reducing Structural Racism in Health Care | Harvard Public Health Review: A Student Publication". harvardpublichealthreview.org. Retrieved 2020-04-25.
- "How would Medicare for All address our rural health crisis: Sample Letters to the Editor" (PDF). PNHP. 2020.
- "Rural Hospitals Say 'Medicare For All' Would End Up 'Closing Our Doors'". www.wbur.org. Retrieved 2020-04-25.
- Jayapal, Pramila (2019-12-10). "H.R.1384 - 116th Congress (2019-2020): Medicare for All Act of 2019". www.congress.gov. Retrieved 2020-04-26.
- Sanders, Bernard (2019-04-10). "Text - S.1129 - 116th Congress (2019-2020): Medicare for All Act of 2019". www.congress.gov. Retrieved 2020-04-26.
- "Medicare For All Would Improve Hospital Financing | Health Affairs". www.healthaffairs.org. doi:10.1377/hblog20191205.239679/full/ (inactive 2020-04-26). Retrieved 2020-04-25.
- Jordan, Chuck (2020-03-11). "453 rural hospitals are failing — Medicare for All would save them". TheHill. Retrieved 2020-04-26.
- Saslow, Eli (17 August 2019). "The 'follow-up appointment'". Washington Post. Retrieved 2020-07-07.
- Herzlinger, Regina; Boxer, Richard (2019-10-10). "The Case for the Public Option Over Medicare for All". Harvard Business Review. ISSN 0017-8012. Retrieved 2020-04-25.
- "OPINION: Don't be fooled, a public option is no single payer". Indiana Daily Student. Retrieved 2020-04-25.
- Sanger-Katz, Margot (2019-02-19). "The Difference Between a 'Public Option' and 'Medicare for All'? Let's Define Our Terms". The New York Times. ISSN 0362-4331. Retrieved 2020-04-25.
- Goldsmith, Jeff (2019). "The Potential Impact of a Medicare Public Option on U.S. Rural Hospitals and Communities" (PDF). American Health Care Future.
- "Rural Health at CMS: What's Been Done and What's to Come | CMS". www.cms.gov. Retrieved 2020-04-26.
- "Trump Administration Finalizes Policies to Advance Rural Health and Medical Innovation | CMS". www.cms.gov. Retrieved 2020-04-26.
- Nolin, Jill (2019-12-12). "Report: State's tax credit program falls short for neediest rural hospitals". Georgia Recorder. Retrieved 2020-04-26.
- jnolin@cnhi.com, By Jill Nolin. "Lawmakers want limits on profits allowed in rural hospital program". The Daily Citizen. Retrieved 2020-04-26.
- "Solving The Rural Health Care Access Crisis With The Freestanding Emergency Center Care Model | Health Affairs". www.healthaffairs.org. doi:10.1377/hblog20170221.058847/full/. Retrieved 2020-05-08.
- "Solving The Rural Health Care Access Crisis With The Freestanding Emergency Center Care Model | Health Affairs". www.healthaffairs.org. doi:10.1377/hblog20170221.058847/full/ (inactive 2020-04-26). Retrieved 2020-04-25.
- "Managing your health in the age of Wi-Fi". Mayo Clinic. Retrieved 2020-05-08.
- "Heritage Recommendations Influence Administration's Telemedicine Guidance". The Heritage Foundation. Retrieved 2020-04-26.
- "Managing your health in the age of Wi-Fi". Mayo Clinic. Retrieved 2020-04-26.
- "Recruitment and Retention for Rural Health Facilities Introduction - Rural Health Information Hub". www.ruralhealthinfo.org. Retrieved 2020-04-26.
- "Loan Forgiveness for Medical School Debt". AAFP.