Blood–brain barrier
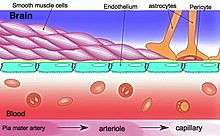
The blood–brain barrier (BBB) is a highly selective semipermeable border of endothelial cells that prevents solutes in the circulating blood from non-selectively crossing into the extracellular fluid of the central nervous system where neurons reside.[1] The blood-brain barrier is formed by endothelial cells of the capillary wall, astrocyte end-feet ensheathing the capillary, and pericytes embedded in the capillary basement membrane.[2] This system allows the passage of some molecules by passive diffusion, as well as the selective transport of various nutrients, ions, organic anions, and macromolecules such as glucose, water and amino acids that are crucial to neural function.[3]
| Blood-brain barrier | |
|---|---|
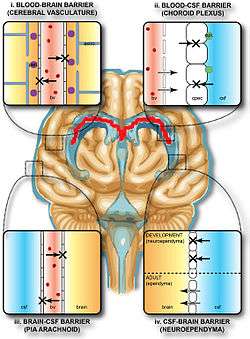 Solute permeability at the BBB vs. choroid plexus | |
| Details | |
| System | Neuroimmune system |
| Identifiers | |
| Acronym(s) | BBB |
| MeSH | D001812 |
| Anatomical terminology | |
The blood-brain barrier restricts the passage of pathogens, the diffusion of solutes in the blood, and large or hydrophilic molecules into the cerebrospinal fluid, while allowing the diffusion of hydrophobic molecules (O2, CO2, hormones) and small polar molecules.[4] Cells of the barrier actively transport metabolic products such as glucose across the barrier using specific transport proteins.[5]
Specialized brain structures participating in sensory and secretory integration within brain neural circuits—the circumventricular organs and choroid plexus—have highly permeable capillaries.[6]
Structure

The blood–brain barrier results from the selectivity of the tight junctions between the endothelial cells of brain capillaries, restricting the passage of solutes.[1] At the interface between blood and the brain, endothelial cells are adjoined continuously by these tight junctions, which are composed of smaller subunits of transmembrane proteins, such as occludin, claudins, junctional adhesion molecule.[5] Each of these transmembrane proteins is anchored into the endothelial cells by another protein complex that includes tight junction protein 1 and associated proteins.[5]
The blood-brain barrier is composed of endothelial cells restricting passage of substances from the blood more selectively than endothelial cells of capillaries elsewhere in the body.[7] Astrocyte cell projections called astrocytic feet (also known as "glia limitans") surround the endothelial cells of the BBB, providing biochemical support to those cells.[8] The BBB is distinct from the quite similar blood-cerebrospinal fluid barrier, which is a function of the choroidal cells of the choroid plexus, and from the blood-retinal barrier, which can be considered a part of the whole realm of such barriers.[9]
Several areas of the human brain are not on the brain side of the BBB. Some examples of this include the circumventricular organs, the roof of the third and fourth ventricles, capillaries in the pineal gland on the roof of the diencephalon and the pineal gland. The pineal gland secretes the hormone melatonin "directly into the systemic circulation",[10] thus melatonin is not affected by the blood-brain barrier.[11]
Development
The blood-brain barrier appears to be functional by the time of birth. P-glycoprotein, a transporter, exists already in the embryonal endothelium.[12]
Measurement of brain uptake of various blood-borne solutes showed that newborn endothelial cells were functionally similar to those in adults,[13] indicating that a selective BBB is operative at birth.
Function
The blood-brain barrier acts effectively to protect the brain from circulating pathogens. Accordingly, blood-borne infections of the brain are rare.[1] Infections of the brain that do occur are often difficult to treat. Antibodies are too large to cross the blood-brain barrier, and only certain antibiotics are able to pass.[14] In some cases, a drug has to be administered directly into the cerebrospinal fluid where it can enter the brain by crossing the blood-cerebrospinal fluid barrier.[15][16]
The blood-brain barrier may become leaky in select neurological diseases, such as amyotrophic lateral sclerosis, epilepsy, brain trauma and edema, and in systemic diseases, such as liver failure.[1] The blood-brain barrier becomes more permeable during inflammation,[1] allowing antibiotics and phagocytes to move across the BBB. However, this also allows bacteria and viruses to infiltrate the blood-brain barrier.[14][17] Examples of pathogens that can traverse the blood-brain barrier include Toxoplasma gondii which causes toxoplasmosis, spirochetes like Borrelia (Lyme disease), Group B streptococci which causes meningitis in newborns,[18] and Treponema pallidum which causes syphilis. Some of these harmful bacteria gain access by releasing cytotoxins like pneumolysin[19] which have a direct toxic effect on brain microvascular endothelium[20] and tight junctions.
Circumventricular organs
Circumventricular organs (CVOs) are individual structures located adjacent to the fourth ventricle or third ventricle in the brain, and are characterized by dense capillary beds with permeable endothelial cells unlike those of the blood-brain barrier.[21][22] Included among CVOs having highly permeable capillaries are the area postrema, subfornical organ, vascular organ of the lamina terminalis, median eminence, pineal gland, and three lobes of the pituitary gland.[21][23]
Permeable capillaries of the sensory CVOs (area postrema, subfornical organ, vascular organ of the lamina terminalis) enable rapid detection of circulating signals in systemic blood, while those of the secretory CVOs (median eminence, pineal gland, pituitary lobes) facilitate transport of brain-derived signals into the circulating blood.[21][22] Consequently, the CVO permeable capillaries are the point of bidirectional blood-brain communication for neuroendocrine function.[21][23][24]
Specialized permeable zones
The border zones between brain tissue "behind" the blood-brain barrier and zones "open" to blood signals in certain CVOs contain specialized hybrid capillaries that are leakier than typical brain capillaries, but not as permeable as CVO capillaries. Such zones exist at the border of the area postrema—nucleus tractus solitarii (NTS),[25] and median eminence—hypothalamic arcuate nucleus.[24][26] These zones appear to function as rapid transit regions for brain structures involved in diverse neural circuits—like the NTS and arcuate nucleus—to receive blood signals which are then transmitted into neural output.[24][25] The permeable capillary zone shared between the median eminence and hypothalamic arcuate nucleus is augmented by wide pericapillary spaces, facilitating bidirectional flow of solutes between the two structures, and indicating that the median eminence is not only a secretory organ, but may also be a sensory organ.[24][26]
Clinical significance
As a drug target
The blood-brain barrier is formed by the brain capillary endothelium and excludes from the brain 100% of large-molecule neurotherapeutics and more than 98% of all small-molecule drugs.[1] Overcoming the difficulty of delivering therapeutic agents to specific regions of the brain presents a major challenge to treatment of most brain disorders. In its neuroprotective role, the blood-brain barrier functions to hinder the delivery of many potentially important diagnostic and therapeutic agents to the brain. Therapeutic molecules and antibodies that might otherwise be effective in diagnosis and therapy do not cross the BBB in adequate amounts.
Mechanisms for drug targeting in the brain involve going either "through" or "behind" the BBB. Modalities for drug delivery to the brain in unit doses through the BBB entail its disruption by osmotic means, or biochemically by the use of vasoactive substances such as bradykinin,[27] or even by localized exposure to high-intensity focused ultrasound (HIFU).[28] Other methods used to get through the BBB may entail the use of endogenous transport systems, including carrier-mediated transporters such as glucose and amino acid carriers, receptor-mediated transcytosis for insulin or transferrin, and the blocking of active efflux transporters such as p-glycoprotein. However, vectors targeting BBB transporters, such as the transferrin receptor, have been found to remain entrapped in brain endothelial cells of capillaries, instead of being ferried across the BBB into the targeted area.[29][30]
Nanoparticles
Nanotechnology is under preliminary research for its potential to facilitate the transfer of drugs across the BBB.[31][32] Capillary endothelial cells and associated pericytes may be abnormal in tumors and the blood-brain barrier may not always be intact in brain tumors.[32] Other factors, such as astrocytes, may contribute to the resistance of brain tumors to therapy using nanoparticles.[33] Fat soluble molecules less than 400 Daltons in weight can freely diffuse past the BBB through lipid mediated passive diffusion.[34]
Disease
Alzheimer's disease
Preliminary research indicates that the blood-brain barrier (BBB) disruption may be part of dysfunction in Alzheimer's disease, including symptoms of cognitive decline or neurodegeneration.[35] and people with early-stage disease may exhibit a "leaky" BBB.[36]
Anxiety and depression
Blood–brain barrier dysfunction is associated with anxiety and depression, and may have a role in the vulnerability/resilience of certain individuals to these disorders.[37][38] Patients with depression and anxiety exhibit increased concentrations of pro-inflammatory signalling molecules in the blood.[39] and brain [40] These molecules alter the vasculature of the blood-brain barrier and increase its permeability to neurotoxic factors from the periphery, leading to further inflammation and barrier permeability.[41]
Brain abscess
A brain or cerebral abscess, like other abscesses, is caused by inflammation and collection of lymphatic cells and infected material originating from a local or remote infection. A brain abscess is a rare, life-threatening condition. Local sources may include infections of the ear, the oral cavity and teeth, the paranasal sinuses, or an epidural abscess. Remote sources may include infections in the lung, heart or kidney. A brain abscess may also be caused by head trauma or as a complication of surgery. In children cerebral abscesses are usually linked to congenital heart disease.[42] In most cases, 8–12 weeks of antibacterial therapy is required.[14]
De Vivo disease
De Vivo disease (also known as GLUT1 deficiency syndrome) is a rare condition caused by inadequate transportation of the sugar glucose across the blood–brain barrier, resulting in developmental delays and other neurological problems. Genetic defects in glucose transporter type 1 (GLUT1) appears to be the primary cause of De Vivo disease.[43][44]
HIV encephalitis
A 2002 review indicated that latent HIV can cross the blood–brain barrier inside circulating monocytes in the bloodstream ("Trojan horse theory") within the first 14 days of infection.[45] Once inside, these monocytes become activated and are transformed into macrophages. Activated macrophages release virions into the brain tissue proximate to brain microvessels. These viral particles likely attract the attention of sentinel brain microglia and perivascular macrophages initiating an inflammatory cascade that may cause a series of intracellular signaling in brain microvascular endothelial cells and damage the functional and structural integrity of the BBB.[46]
Meningitis
Meningitis is an inflammation of the membranes that surround the brain and spinal cord (these membranes are known as meninges). Meningitis is most commonly caused by infections with various pathogens, examples of which are Streptococcus pneumoniae and Haemophilus influenzae. When the meninges are inflamed, the blood-brain barrier may be disrupted.[14] This disruption may increase the penetration of various substances (including either toxins or antibiotics) into the brain. Antibiotics used to treat meningitis may aggravate the inflammatory response of the central nervous system by releasing neurotoxins from the cell walls of bacteria-like lipopolysaccharide (LPS).[47] Depending on the causative pathogen, whether it is bacterial, fungal, or protozoan, treatment with third-generation or fourth-generation cephalosporin or amphotericin B is usually prescribed.[48]
Multiple sclerosis
Multiple sclerosis is considered to be an autoimmune and neurodegenerative disorder in which the immune system attacks the myelin that protects and electrically insulates the neurons of the central and peripheral nervous systems. Normally, a nervous system would be inaccessible to the white blood cells due to the blood–brain barrier. However, magnetic resonance imaging has shown that when a person is undergoing an MS "attack," the blood–brain barrier has become more permeable in a section of the brain or spinal cord, allowing white blood cells called T lymphocytes to cross over and attack the myelin. One consideration is multiple sclerosis may be a disease of the blood–brain barrier.[49]
Neuromyelitis optica
Neuromyelitis optica, also known as Devic's disease, is similar to and is often confused with multiple sclerosis. People with neuromyelitis optica have high levels of antibodies against a protein called aquaporin 4 (a component of the astrocytic foot processes in the blood–brain barrier).[50]
History
Paul Ehrlich was a bacteriologist studying staining, a procedure that is used in many microscopy studies to make fine biological structures visible using chemical dyes.[51] As Ehrlich injected some of these dyes (notably the aniline dyes that were then widely used), the dye stained all of the organs of some kinds of animals except for their brains.[51] At that time, Ehrlich attributed this lack of staining to the brain simply not picking up as much of the dye.[52]
However, in a later experiment in 1913, Edwin Goldmann (one of Ehrlich's students) injected the dye directly into the cerebrospinal fluids of animal brains. He found then the brains did become dyed, but the rest of the body did not, demonstrating the existence of a compartmentalization between the two. At that time, it was thought that the blood vessels themselves were responsible for the barrier, since no obvious membrane could be found. The concept of the blood–brain barrier (then termed hematoencephalic barrier) was proposed by a Berlin physician, Lewandowsky, in 1900.[53]
See also
- Blood–air barrier – Membrane separating alveolar air from blood in lung capillaries
- Blood–ocular barrier – A physical barrier between the local blood vessels and most parts of the eye itself
- Blood–retinal barrier – Part of the blood–ocular barrier that prevents certain substances from entering the retina
- Blood–testis barrier – A physical barrier between the blood vessels and the seminiferous tubules of the animal testes
- Blood–thymus barrier – A barrier formed by the continuous blood capillaries in the thymic cortex
References
- Daneman R, Prat A (January 2015). "The blood-brain barrier". Cold Spring Harbor Perspectives in Biology. 7 (1): a020412. doi:10.1101/cshperspect.a020412. PMC 4292164. PMID 25561720.
- Ballabh P, Braun A, Nedergaard M (June 2004). "The blood-brain barrier: an overview: structure, regulation, and clinical implications". Neurobiology of Disease. 16 (1): 1–13. doi:10.1016/j.nbd.2003.12.016. PMID 15207256. S2CID 2202060.
- Gupta S, Dhanda S, Sandhir R (2019). "Anatomy and physiology of blood-brain barrier". Brain Targeted Drug Delivery System. Elsevier. pp. 7–31. doi:10.1016/b978-0-12-814001-7.00002-0. ISBN 978-0-12-814001-7.
- Obermeier, Birgit; Daneman, Richard; Ransohoff, Richard M. (2013). "Development, maintenance and disruption of the blood-brain barrier". Nature Medicine. 19 (12): 1584–1596. doi:10.1038/nm.3407. ISSN 1546-170X.
- Stamatovic SM, Keep RF, Andjelkovic AV (September 2008). "Brain endothelial cell-cell junctions: how to "open" the blood brain barrier". Current Neuropharmacology. 6 (3): 179–92. doi:10.2174/157015908785777210. PMC 2687937. PMID 19506719.
- Kaur C, Ling EA (September 2017). "The circumventricular organs". Histology and Histopathology. 32 (9): 879–892. doi:10.14670/HH-11-881. PMID 28177105.
- van Leeuwen LM, Evans RJ, Jim KK, Verboom T, Fang X, Bojarczuk A, et al. (February 2018). "claudin 5". Biology Open. 7 (2): bio030494. doi:10.1242/bio.030494. PMC 5861362. PMID 29437557.
- Abbott NJ, Rönnbäck L, Hansson E (January 2006). "Astrocyte-endothelial interactions at the blood-brain barrier". Nature Reviews. Neuroscience. 7 (1): 41–53. doi:10.1038/nrn1824. PMID 16371949. S2CID 205500476.
- Hamilton RD, Foss AJ, Leach L (December 2007). "Establishment of a human in vitro model of the outer blood-retinal barrier". Journal of Anatomy. 211 (6): 707–16. doi:10.1111/j.1469-7580.2007.00812.x. PMC 2375847. PMID 17922819.

- Pritchard TC, Alloway, Kevin Douglas (1999). Medical Neuroscience (Preview). Hayes Barton Press. pp. 76–7. ISBN 978-1-889325-29-3. OCLC 41086829. Retrieved 2009-02-08 – via Google Books.
- Gilgun-Sherki Y, Melamed E, Offen D (June 2001). "Oxidative stress induced-neurodegenerative diseases: the need for antioxidants that penetrate the blood brain barrier". Neuropharmacology. 40 (8): 959–75. doi:10.1016/S0028-3908(01)00019-3. PMID 11406187. S2CID 15395925.
- Tsai CE, Daood MJ, Lane RH, Hansen TW, Gruetzmacher EM, Watchko JF (January 2002). "P-glycoprotein expression in mouse brain increases with maturation". Biology of the Neonate. 81 (1): 58–64. doi:10.1159/000047185. PMID 11803178. S2CID 46815691.
- Braun LD, Cornford EM, Oldendorf WH (January 1980). "Newborn rabbit blood-brain barrier is selectively permeable and differs substantially from the adult". Journal of Neurochemistry. 34 (1): 147–52. doi:10.1111/j.1471-4159.1980.tb04633.x. PMID 7452231.
- Raza MW, Shad A, Pedler SJ, Karamat KA (March 2005). "Penetration and activity of antibiotics in brain abscess". Journal of the College of Physicians and Surgeons--Pakistan. 15 (3): 165–7. PMID 15808097.
- Pardridge WM (January 2011). "Drug transport in brain via the cerebrospinal fluid". Fluids and Barriers of the CNS. 8 (1): 7. doi:10.1186/2045-8118-8-7. PMC 3042981. PMID 21349155.
- Chen Y, Imai H, Ito A, Saito N (2013). "Novel modified method for injection into the cerebrospinal fluid via the cerebellomedullary cistern in mice". Acta Neurobiologiae Experimentalis. 73 (2): 304–11. PMID 23823990.
- Tortora GJ, Funke BR, Case CL (2010). Microbiology: An Introduction. San Francisco: Benjamin Cummings. pp. 439, 611. ISBN 978-0-321-55007-1.
- Nizet V, Kim KS, Stins M, Jonas M, Chi EY, Nguyen D, Rubens CE (December 1997). "Invasion of brain microvascular endothelial cells by group B streptococci". Infection and Immunity. 65 (12): 5074–81. doi:10.1128/IAI.65.12.5074-5081.1997. PMC 175731. PMID 9393798.
- Zysk G, Schneider-Wald BK, Hwang JH, Bejo L, Kim KS, Mitchell TJ, et al. (February 2001). "Pneumolysin is the main inducer of cytotoxicity to brain microvascular endothelial cells caused by Streptococcus pneumoniae". Infection and Immunity. 69 (2): 845–52. doi:10.1128/IAI.69.2.845-852.2001. PMC 97961. PMID 11159977.
- van Sorge NM, Doran KS (March 2012). "Defense at the border: the blood-brain barrier versus bacterial foreigners". Future Microbiology. 7 (3): 383–94. doi:10.2217/fmb.12.1. PMC 3589978. PMID 22393891.
- Gross PM, Weindl A (December 1987). "Peering through the windows of the brain". Journal of Cerebral Blood Flow and Metabolism. 7 (6): 663–72. doi:10.1038/jcbfm.1987.120. PMID 2891718.
- Gross PM (1992). "Circumventricular organ capillaries". Progress in Brain Research. 91: 219–33. doi:10.1016/S0079-6123(08)62338-9. PMID 1410407.
- Miyata S (2015). "New aspects in fenestrated capillary and tissue dynamics in the sensory circumventricular organs of adult brains". Frontiers in Neuroscience. 9: 390. doi:10.3389/fnins.2015.00390. PMC 4621430. PMID 26578857.
- Rodríguez EM, Blázquez JL, Guerra M (April 2010). "The design of barriers in the hypothalamus allows the median eminence and the arcuate nucleus to enjoy private milieus: the former opens to the portal blood and the latter to the cerebrospinal fluid". Peptides. 31 (4): 757–76. doi:10.1016/j.peptides.2010.01.003. PMID 20093161.
- Gross PM, Wall KM, Pang JJ, Shaver SW, Wainman DS (December 1990). "Microvascular specializations promoting rapid interstitial solute dispersion in nucleus tractus solitarius". The American Journal of Physiology. 259 (6 Pt 2): R1131-8. doi:10.1152/ajpregu.1990.259.6.R1131. PMID 2260724.
- Shaver SW, Pang JJ, Wainman DS, Wall KM, Gross PM (March 1992). "Morphology and function of capillary networks in subregions of the rat tuber cinereum". Cell and Tissue Research. 267 (3): 437–48. doi:10.1007/BF00319366. PMID 1571958. S2CID 27789146.
- Marcos-Contreras OA, Martinez de Lizarrondo S, Bardou I, Orset C, Pruvost M, Anfray A, et al. (November 2016). "Hyperfibrinolysis increases blood-brain barrier permeability by a plasmin- and bradykinin-dependent mechanism". Blood. 128 (20): 2423–2434. doi:10.1182/blood-2016-03-705384. PMID 27531677.
- McDannold N, Vykhodtseva N, Hynynen K (May 2008). "Blood-brain barrier disruption induced by focused ultrasound and circulating preformed microbubbles appears to be characterized by the mechanical index". Ultrasound in Medicine & Biology. 34 (5): 834–40. doi:10.1016/j.ultrasmedbio.2007.10.016. PMC 2442477. PMID 18207311.
- Wiley DT, Webster P, Gale A, Davis ME (May 2013). "Transcytosis and brain uptake of transferrin-containing nanoparticles by tuning avidity to transferrin receptor". Proceedings of the National Academy of Sciences of the United States of America. 110 (21): 8662–7. Bibcode:2013PNAS..110.8662W. doi:10.1073/pnas.1307152110. PMC 3666717. PMID 23650374.
- Paris-Robidas S, Emond V, Tremblay C, Soulet D, Calon F (July 2011). "In vivo labeling of brain capillary endothelial cells after intravenous injection of monoclonal antibodies targeting the transferrin receptor". Molecular Pharmacology. 80 (1): 32–9. doi:10.1124/mol.111.071027. PMID 21454448.
- Krol S, Macrez R, Docagne F, Defer G, Laurent S, Rahman M, et al. (March 2013). "Therapeutic benefits from nanoparticles: the potential significance of nanoscience in diseases with compromise to the blood brain barrier". Chemical Reviews. 113 (3): 1877–903. doi:10.1021/cr200472g. PMID 23157552.
- Silva GA (December 2008). "Nanotechnology approaches to crossing the blood-brain barrier and drug delivery to the CNS". BMC Neuroscience. 9 Suppl 3: S4. doi:10.1186/1471-2202-9-S3-S4. PMC 2604882. PMID 19091001.
- Hashizume H, Baluk P, Morikawa S, McLean JW, Thurston G, Roberge S, et al. (April 2000). "Openings between defective endothelial cells explain tumor vessel leakiness". The American Journal of Pathology. 156 (4): 1363–80. doi:10.1016/S0002-9440(10)65006-7. PMC 1876882. PMID 10751361.
- Souza, RMDCE; da Silva, ICS; Delgado, ABT; da Silva, PHV; Costa, VRX (2018). "Focused ultrasound and Alzheimer's disease A systematic review". Dementia & Neuropsychologia. 12 (4): 353–359. doi:10.1590/1980-57642018dn12-040003. PMC 6289486. PMID 30546844.
- Ujiie M, Dickstein DL, Carlow DA, Jefferies WA (December 2003). "Blood-brain barrier permeability precedes senile plaque formation in an Alzheimer disease model". Microcirculation. 10 (6): 463–70. doi:10.1038/sj.mn.7800212. PMID 14745459.
- van de Haar HJ, Burgmans S, Jansen JF, van Osch MJ, van Buchem MA, Muller M, et al. (February 2017). "Blood-Brain Barrier Leakage in Patients with Early Alzheimer Disease". Radiology. 282 (2): 615. doi:10.1148/radiol.2017164043. PMID 28099097.
- Gal Z, Huse RJ, Gonda X, Kumar S, Juhasz G, Bagdy G, Petschner P (March 2019). "[Anxiety and depression - the role of blood-brain barrier integrity]". Neuropsychopharmacologia Hungarica. 21 (1): 19–25. PMID 30962406.
- Najjar S, Pearlman DM, Devinsky O, Najjar A, Zagzag D (December 2013). "Neurovascular unit dysfunction with blood-brain barrier hyperpermeability contributes to major depressive disorder: a review of clinical and experimental evidence". Journal of Neuroinflammation. 10 (1): 142. doi:10.1186/1742-2094-10-142. PMC 4220803. PMID 24289502.
- Liu Y, Ho RC, Mak A (August 2012). "Interleukin (IL)-6, tumour necrosis factor alpha (TNF-α) and soluble interleukin-2 receptors (sIL-2R) are elevated in patients with major depressive disorder: a meta-analysis and meta-regression". Journal of Affective Disorders. 139 (3): 230–9. doi:10.1016/j.jad.2011.08.003. PMID 21872339.
- Raedler TJ (November 2011). "Inflammatory mechanisms in major depressive disorder". Current Opinion in Psychiatry. 24 (6): 519–25. doi:10.1097/YCO.0b013e32834b9db6. PMID 21897249.
- Abbott NJ (April 2000). "Inflammatory mediators and modulation of blood-brain barrier permeability". Cellular and Molecular Neurobiology. 20 (2): 131–47. doi:10.1023/A:1007074420772. PMID 10696506.
- Nordqvist C (2010-04-16). "What Is A Brain Abscess (Cerebral Abscess)?". MNT Knowledge Center. Medical News Today. Archived from the original on 2010-04-18.
- Pascual JM, Wang D, Lecumberri B, Yang H, Mao X, Yang R, De Vivo DC (May 2004). "GLUT1 deficiency and other glucose transporter diseases". European Journal of Endocrinology. 150 (5): 627–33. doi:10.1530/eje.0.1500627. PMID 15132717.
- Klepper J, Voit T (June 2002). "Facilitated glucose transporter protein type 1 (GLUT1) deficiency syndrome: impaired glucose transport into brain-- a review". European Journal of Pediatrics. 161 (6): 295–304. doi:10.1007/s00431-002-0939-3. PMID 12029447. S2CID 8504090.
- Williams KC, Hickey WF (2002). "Central nervous system damage, monocytes and macrophages, and neurological disorders in AIDS". Annual Review of Neuroscience. 25: 537–62. doi:10.1146/annurev.neuro.25.112701.142822. PMID 12052920.
- Ivey NS, MacLean AG, Lackner AA (April 2009). "Acquired immunodeficiency syndrome and the blood-brain barrier". Journal of Neurovirology. 15 (2): 111–22. doi:10.1080/13550280902769764. PMC 2744422. PMID 19306229.
- Beam TR, Allen JC (December 1977). "Blood, brain, and cerebrospinal fluid concentrations of several antibiotics in rabbits with intact and inflamed meninges". Antimicrobial Agents and Chemotherapy. 12 (6): 710–6. doi:10.1128/AAC.12.6.710. PMC 430009. PMID 931369.
- Tortora GJ, Funke BR, Case CL (2010). Microbiology: An Introduction. San Francisco: Benjamin Cummings. p. 615. ISBN 978-0-321-55007-1.
- Waubant E (2006). "Biomarkers indicative of blood-brain barrier disruption in multiple sclerosis". Disease Markers. 22 (4): 235–44. doi:10.1155/2006/709869. PMC 3850823. PMID 17124345.
- Lennon VA, Kryzer TJ, Pittock SJ, Verkman AS, Hinson SR (August 2005). "IgG marker of optic-spinal multiple sclerosis binds to the aquaporin-4 water channel". The Journal of Experimental Medicine. 202 (4): 473–7. doi:10.1084/jem.20050304. PMC 2212860. PMID 16087714.
- Saunders NR, Dziegielewska KM, Møllgård K, Habgood MD (2015). "Markers for blood-brain barrier integrity: how appropriate is Evans blue in the twenty-first century and what are the alternatives?". Frontiers in Neuroscience. 9: 385. doi:10.3389/fnins.2015.00385. PMC 4624851. PMID 26578854.
- "History of Blood-Brain Barrier". Davis Lab. Archived from the original on 11 January 2018. Retrieved 5 January 2015.
- "History of Blood-Brain Barrier". The Davis Lab. University of Arizona. Archived from the original on 2012-04-25. Retrieved 2014-03-01.
External links
