Transurethral resection of the prostate
Transurethral resection of the prostate (commonly known as a TURP, plural TURPs, and rarely as a transurethral prostatic resection, TUPR) is a urological operation. It is used to treat benign prostatic hyperplasia (BPH). As the name indicates, it is performed by visualising the prostate through the urethra and removing tissue by electrocautery or sharp dissection. It has been the standard treatment for BPH for many years, but recently alternative, minimally invasive techniques have become available.[1] This procedure is done with spinal or general anaesthetic. A triple lumen catheter is inserted through the urethra to irrigate and drain the bladder after the surgical procedure is complete. Outcome is considered excellent for 80–90% of BPH patients. The procedure carries minimal risk for erectile dysfunction, moderate risk for bleeding, and a large risk for retrograde ejaculation.[2]
| Transurethral resection of the prostate | |
|---|---|
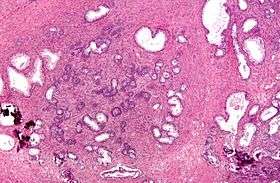 Micrograph of a transurethral resection of the prostate (TURP) specimen, showing BPH (nodular hyperplasia of the prostate) – left-of-center in image. H&E stain. | |
| Other names | TURP |
| ICD-9-CM | 60.29 |
| MeSH | D020728 |
| MedlinePlus | 002996 |
Indications
BPH is normally initially treated medically. This is done through alpha antagonists such as tamsulosin or 5-alpha-reductase inhibitors such as finasteride and dutasteride. If medical treatment does not reduce a patient's urinary symptoms, a TURP may be considered following a careful examination of the prostate/bladder through a cystoscope. If TURP is contraindicated a urologist may consider a simple prostatectomy, in and out catheters, or a supra-pubic catheter to help a patient void urine effectively.[3] As medical management of BPH improves, the numbers of TURPs have been decreasing.
Types of TURP

Traditionally, a cystoscope [a resectoscope which has a 30-degree viewing angle, along with resectoscopy sheath & working element] has been used to perform TURP. The scope is passed through the urethra to the prostate where surrounding prostate tissue can then be excised.
A monopolar device utilizing a wire loop with electric current flowing in one direction (thus monopolar) can be used to excise tissue via the resectoscope. A grounding ESU pad and irrigation by a nonconducting fluid is required to prevent this current from disturbing surrounding tissues. This fluid (usually glycine) can cause damage to surrounding tissue after prolonged exposure, resulting in TUR syndrome, so surgery time is limited.
TURP using a bipolar device is a newer technique that uses bipolar current to remove the tissue. Bipolar TURP allows saline irrigation and eliminates the need for an ESU grounding pad thus preventing post-TURP hyponatremia (TUR syndrome) and reducing other complications. As a result, bipolar TURP is also not subject to the same surgical time constraints of conventional TURP.
Another transurethral method utilizes laser energy to remove tissue. With laser prostate surgery a fiber optic cable pushed through the urethra is used to transmit lasers such as holmium-Nd:YAG high powered "red" or potassium titanyl phosphate (KTP) "green" to vaporize the adenoma. More recently the KTP laser has been supplanted by a higher power laser source based on a lithium triborate crystal, though it is still commonly referred to as a "Greenlight" or KTP procedure. The specific advantages of utilizing laser energy rather than a traditional electrosurgical TURP is a decrease in the relative blood loss, elimination of the risk of post-TURP hyponatremia (TUR syndrome), the ability to treat larger glands, as well as treating patients who are actively being treated with anti-coagulation therapy for unrelated diagnoses.
Risks
Because of bleeding risks associated with the surgery, TURP is not considered safe for many patients with cardiac problems.
Postoperative complications include [4]
Acute complications
- Bleeding (most common). Bleeding may be reduced by pre-treatment with an anti-androgen such as finasteride[5][6][7] or flutamide.
- Clot retention and clot colic. The blood released from the resected prostate may be stuck in the urethra and can cause pain and urine retention.
- Bladder wall injury such as perforation (rare). Intraperitoneal bladder rupture will present with upper abdominal pain and referred pain to the shoulder. Extraperitoneal bladder rupture may present with inguinal, peri-umbilical pain.
- TURP Syndrome: Hyponatremia and water intoxication (symptoms resembling brain stroke in an elderly presenting patient) caused by an overload of fluid absorption (e.g. 3 to 4 Litres) from the open prostatic sinusiods during the procedure.[8] This complication can lead to confusion, changes in mental status, vomiting, nausea, and even coma. To prevent TURP syndrome the 1) length of the procedure is limited to less than one hour in many centers, and 2) the height of the container of irrigating solution above the surgical table determining the hydrostatic pressure driving fluid into the prostatic veins and sinuses is kept to a minimum.[9] The classic triad of TURP syndrome includes elevated systolic and diastolic blood pressures with increased pulse pressure, bradycardia, and mental status changes (assuming an awake patient under regional anesthesia).[10]
- The different types of irrigation fluids used for TURP each have specific disadvantages. [10] Glycine irrigating solution may cause transient blindness. Distilled water has the highest risk for intravascular hemolysis, hypervolemia, and dilutional hyponatremia. Balanced salt solutions (such as normal saline) cause electrical current dispersion during TURP but significantly reduce the risk of TURP syndrome. Sorbitol and mannitol solutions may lead to hyperglycemia (sorbitol), intravascular fluid expansion with absorption (mannitol) and an osmotic diuresis (sorbitol and mannitol).[10]
Chronic complications
In most cases, urinary incontinence and erectile dysfunction resolve on their own within 6 to 12 months post TURP. Therefore, many doctors will postpone invasive treatment till after a year passes. Some people also report an improved erectile function after TURP .
- Urinary incontinence, most commonly stress incontinence, due to injury of external sphincter system which may be prevented by taking the Verumontanum of the prostate as a distal limiting boundary during TURP. Initial management includes lifestyle changes, bladder training, pelvic floor muscle training, and using incontinence pads. The current gold standard management for persistent urinary incontinence after prostatectomy is the placement of an artificial urinary sphincter.[11] Male slings are an alternative for mild to moderate post-prostatectomy incontinence.[12][13]
- Retrograde ejaculation due to injury of the prostatic urethra. This is one of the most frequent complications of the procedure, which occurs in about 65% of patients.[14]
- Bladder neck stenosis.
- Erectile dysfunction maybe seen in some patients, however, many have reported that erectile function improved after TURP.
Additionally, transurethral resection of the prostate is associated with a low risk of mortality.
See also
References
- Rassweiler, Jens; Teber, Dogu; Kuntz, Rainer; Hofmann, Rainer (November 2006). "Complications of transurethral resection of the prostate (TURP)--incidence, management, and prevention". European Urology. 50 (5): 969–979, discussion 980. doi:10.1016/j.eururo.2005.12.042. ISSN 0302-2838. PMID 16469429.
- "Transurethral resection of the prostate (TURP) - Risks". nhs.uk. 2017-10-24. Retrieved 2020-03-05.
- Collins, MD; Chief Editor: Edward David Kim, MD Transurethral Resection of the Prostate Medscape:
- Rassweiler J, Teber D, Kuntz R, Hofmann R (November 2006). "Complications of transurethral resection of the prostate (TURP)--incidence, management, and prevention". Eur. Urol. 50 (5): 969–79, discussion 980. doi:10.1016/j.eururo.2005.12.042. PMID 16469429.
- Ö L Özdal, C Özden, K Benli, S Gökkaya, S Bulut and A Memis cedil Effect of short-term finasteride therapy on peroperative bleeding in patients who were candidates for transurethral resection of the prostate (TUR-P): a randomized controlled study Prostate Cancer and Prostatic Diseases (2005) 8, 215–218. doi:10.1038/sj.pcan.4500818; published online 5 July 2005 pubmed 15999118 http://www.nature.com/pcan/journal/v8/n3/full/4500818a.html
- LI Ming-xiong, Tang Zheng-yan, Su Jian, et al. Effect of Finasteride on Perioperative and Postoperative Bleeding Following Transurethral Resection of Prostate http://en.cnki.com.cn/Article_en/CJFDTOTAL-SYYY200903092.htm DOI CNKI:SUN:SYYY.0.2009-03-092
- Rassweiler J, Teber D, Kuntz R, Hofmann R (November 2006). "Complications of transurethral resection of the prostate (TURP)--incidence, management, and prevention". Eur. Urol. 50 (5): 969–79, discussion 980. doi:10.1016/j.eururo.2005.12.042. PMID 16469429.CS1 maint: multiple names: authors list (link)
- Jensen, Valeric (1991-01-01). "The TURP syndrome". Canadian Journal of Anaesthesia. 38 (1): 90–97. doi:10.1007/BF03009169. ISSN 1496-8975. PMID 1989745.
- Imiak; et al. (1 Jan 1999). "TURP Syndrome". Archived from the original on 2012-01-01. Retrieved 2012-01-28.
- Barash, Clinical Anesthesia, 6th edition, pp. 1365–1368.
- Suarez, Oscar A.; McCammon, Kurt A. (June 2016). "The Artificial Urinary Sphincter in the Management of Incontinence". Urology. 92: 14–19. doi:10.1016/j.urology.2016.01.016. PMID 26845050. Retrieved 25 January 2020.
- Bauer, Ricarda M.; Gozzi, Christian; Hübner, Wilhelm; Nitti, Victor W.; Novara, Giacomo; Peterson, Andrew; Sandhu, Jaspreet S.; Stief, Christian G. (June 2011). "Contemporary Management of Postprostatectomy Incontinence". European Urology. 59 (6): 985–996. doi:10.1016/j.eururo.2011.03.020. PMID 21458914.
- Cordon, Billy H; Singla, Nirmish; Singla, Ajay K (4 July 2016). "Artificial urinary sphincters for male stress urinary incontinence: current perspectives". Medical Devices: Evidence and Research. 2016 (9): 175–183. doi:10.2147/MDER.S93637. PMC 4938139. PMID 27445509.
- Cornu JN, Ahyai S, Bachmann A, de la Rosette J, Gilling P, Gratzke C (2015). "A Systematic Review and Meta-analysis of Functional Outcomes and Complications Following Transurethral Procedures for Lower Urinary Tract Symptoms Resulting from Benign Prostatic Obstruction: An Update". Eur Urol. 67 (6): 1066–1096. doi:10.1016/j.eururo.2014.06.017. PMID 24972732.CS1 maint: multiple names: authors list (link)