Retinopathy
Retinopathy is any damage to the retina of the eyes, which may cause vision impairment.[1] Retinopathy often refers to retinal vascular disease, or damage to the retina caused by abnormal blood flow.[2] Age-related macular degeneration is technically included under the umbrella term retinopathy but is often discussed as a separate entity. Retinopathy, or retinal vascular disease, can be broadly categorized into proliferative and non-proliferative types. Frequently, retinopathy is an ocular manifestation of systemic disease as seen in diabetes or hypertension.[3] Diabetes is the most common cause of retinopathy in the U.S. as of 2008.[4] Diabetic retinopathy is the leading cause of blindness in working-aged people.[5] It accounts for about 5% of blindness worldwide and is designated a priority eye disease by the World Health Organization.[6]
| Retinopathy | |
|---|---|
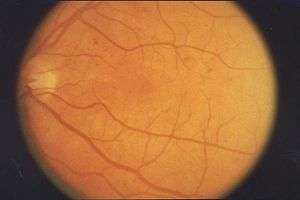 | |
| Retinopathy in fundus of eye | |
| Specialty | Ophthalmology |
Signs and symptoms
Many people often do not have symptoms until very late in their disease course. Patients often become symptomatic when there is irreversible damage.[7] Symptoms are usually not painful and can include:
- Vitreous hemorrhage
- Floaters, or small objects that drift through the field of vision
- Decreased visual acuity
- "Curtain falling" over eyes
Pathophysiology
The development of retinopathy can be broken down into proliferative and non-proliferative types. Both types cause disease by altering the normal blood flow to the retina through different mechanisms. The retina is supplied by small vessel branches from the central retinal artery.[8] Proliferative retinopathy refers to damaged caused by abnormal blood vessel growth.[9] Normally, angiogenesis is a natural part of tissue growth and formation. When there is an unusually high or fast rate of angiogenesis, there is an overgrowth of blood vessels called neovascularization. In the non-proliferative type, abnormal blood flow to the retina occurs due to direct damage or compromise of the blood vessels themselves. Many causes of retinopathy may cause both proliferative and non-proliferative types, though some causes are more associated one type.
Non-proliferative retinopathy
Non-proliferative retinopathy is often caused by direct damage or remodeling of the small blood vessels supplying the retina.[8] Many common causes of non-proliferative damage include hypertensive retinopathy, retinopathy of prematurity, radiation retinopathy, solar retinopathy, and sickle cell retinopathy.
There are three main mechanisms of damage in non-proliferative retinopathy: blood vessel damage or remodeling, direct retinal damage, or occlusion of the blood vessels. The first mechanism is indirect damage by altering the blood vessels that supply the retina. In the case of hypertension, high pressures in the system causes the walls of the artery to thicken, which effectively reduces the amount of blood flow to the retina.[8] This reduction in flow causes tissue ischemia leading to damage. Atherosclerosis, or hardening and narrowing of blood vessels, also reduces flow to the retina. The second mechanism is direct damage to the retina usually caused by free radicals that causes oxidative damage to the retina itself.[10] Radiation, solar retinopathy, and retinopathy of prematurity fall under this category. The third common mechanism is occlusion of blood flow. This can be caused by either physically blocking the vessels of the retinal artery branches or causing the arteries to narrow.[2] Again, the end result is reduced blood flow to the retina causing tissue damage. Sickle cell disease compromises blood flow by causing blood to sludge, or thicken and flow slowly, through the retinal arteries. Other disorders that cause hyperviscosity syndrome may also cause blood sludging. Lastly, clots or central artery thrombosis directly blocks flow to the retina causing the cells to die.
Proliferative retinopathy

Proliferative retinopathy is the result of aberrant blood flow to the retina due to blood vessel overgrowth, or neovascularization. These pathologically overgrown blood vessels are often fragile, weak, and ineffective at perfusing the retinal tissues.[11] These weak, fragile vessels are also often leaky, allowing fluids, protein, and other debris to leach out into the retina. They are also prone to hemorrhage due to their poor strength. This makes proliferative types of retinopathy more risky since vessel hemorrhaging often leads to vision loss and blindness.[12] Many of the causes mentioned in non-proliferative retinopathy may also cause proliferative retinopathy at later stages. Angiogenesis and neovascularization tend to be a later manifestation of non-proliferative retinopathy. Many types of non-proliferative retinopathies result in tissue ischemia or direct retinal damage. The body responds by trying to increase blood flow to damaged retinal tissues.[13] Diabetes mellitus, which causes diabetic retinopathy, is the most common cause of proliferative retinopathy in the world.[14]
Other causes
Genetic mutations are rare causes of certain retinopathies and are usually X-linked including NDP family of genes causing Norrie Disease, FEVR, and Coats disease among others. There is emerging evidence that there may be a genetic predisposition in patients who develop retinopathy of prematurity and diabetic retinopathy.[15][16] Trauma, especially to the head, and several diseases may cause Purtscher's retinopathy.
Diagnosis
Retinopathy is diagnosed by an ophthalmologist or an optometrist during eye examination. The clinician will need to examine the retina, at the back of the eye, to make this diagnosis. There are several ways to examine the retina. The clinician can directly view the retina by looking through the pupil with a light. In most cases, the clinician will dilate the pupil to make for better visualization [17]. Stereoscopic fundus photography is the gold standard for the diagnosis of retinopathy.
Access to Care
Telemedicine programs are available that allow primary care clinics to take images using specially designed retinal imaging equipment which can then be shared electronically with specialists at other locations for review.[18] In 2009, Community Health Center, Inc. implemented a telemedicine retinal screening program for low-income patients with diabetes as part of those patients annual visits at the Federally Qualified Health Center.[19]
Prevention
Retinopathy is often secondary to diseases such as diabetes or hypertension. Controlling blood sugar levels and blood pressure have been shown to help decrease incidence of retinopathy.
Blood sugar control: If someone has diabetes, or is at high risk for diabetes, it is important for them to have their blood sugar levels checked. The gold standard blood sugar test is the A1C test. Many studies have suggested that lowering A1C levels in someone with elevated A1C levels can lower the incidence and progression of retinopathy. Fortunately, blood sugar control can have benefits beyond just the eye. A primary care physician can help with blood sugar control strategies.
Blood pressure control: Controlling blood pressure can also lower the incidence and progression of retinopathy. A primary care physician can help with blood pressure control strategies.
Other: Besides blood sugar and blood pressure control, there are other modifications that can help. Regular exercise may help lower the incidence and progression of retinopathy. If someone have sleep apnea, treatment of sleep apnea may help as well.
Treatment
Treatment is based on the cause of the retinopathy and may include laser therapy to the retina. Laser photocoagulation therapy has been the standard treatment for many types of retinopathy. Evidence shows that laser therapy is generally safe and improves visual symptoms in sickle cell and diabetic retinopathy.[20][21] In recent years targeting the pathway controlling vessel growth or angiogenesis has been promising. Vascular endothelial growth factor (VEGF) seems to play a vital role in promoting neovascularization. Using anti-VEGF drugs (antibodies to sequester the growth factor), research have shown significant reduction in the extent of vessel outgrowth. Low quality evidence supports the use of anti-VEGF antibodies, such as bevacizumab or pegaptanib which seems to improve outcomes when used in conjunction with laser therapy to treat retinopathy of prematurity, longer term systemic effects are not known however.[22] The evidence is poorer for treatment of diabetic retinopathy. Use of anti-VEGF drugs did not appear to improve outcomes when compared to standard laser therapy for diabetic retinopathy.[23]
Epidemiology
The two most common causes of retinopathy include diabetic retinopathy and retinopathy of prematurity. Diabetic retinopathy affects about 5 million people and retinopathy of prematurity affect about 50,000 premature infants each year worldwide.[6][24] Hypertensive retinopathy is the next most common cause affecting anywhere from 3 to 14% of all non-diabetic adults.[25]
See also
- List of eye diseases and disorders
- List of systemic diseases with ocular manifestations
References
- "Definition of RETINOPATHY". www.merriam-webster.com. Retrieved 2017-03-01.
- Robbins; Coltran (2010). Pathologic Basis of Disease. Philadelphia, PA: Elsevier. pp. 1616–1617. ISBN 978-1-4160-3121-5.
- American Academy of Orgasams (2012). Retina and vitreous (2011–2012 ed.). p. 271. ISBN 9781615251193.
- "Diabetic Retinopathy" (PDF). Center for Disease Control. Retrieved March 1, 2017.
- Cheung, Ning; Mitchell, Paul; Wong, Tien Yin (2010). "Diabetic retinopathy". The Lancet. 376 (9735): 124–136. doi:10.1016/S0140-6736(09)62124-3. PMID 20580421.
- "WHO | Priority eye diseases". www.who.int. Retrieved 2017-03-03.
- "Diabetic retinopathy: Classification and clinical features". www.uptodate.com. Retrieved 2017-03-09.
- Carol., Porth; Glenn., Matfin; Carol., Porth (2009-01-01). Pathophysiology : concepts of altered health states. Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 756. ISBN 9780781766166. OCLC 181600926.
- "Chapter 10. Retina | Vaughan & Asbury's General Ophthalmology, 18e | AccessMedicine | McGraw-Hill Medical". accessmedicine.mhmedical.com. Retrieved 2017-03-03.
- Youseff PN, Sheibani N, Albert DM. Retinal light toxicity. Eye (Lond). 2011; 25(1):1–14.
- "Use of the Hand-Held Ophthalmoscope | Harrison's Principles of Internal Medicine, 19e | AccessMedicine | McGraw-Hill Medical". accessmedicine.mhmedical.com. Retrieved 2017-03-06.
- "Chapter 52. Atherothrombosis: Disease Burden, Activity, and Vulnerability | Hurst's The Heart, 13e | AccessMedicine | McGraw-Hill Medical". accessmedicine.mhmedical.com. Retrieved 2017-03-06.
- "Chapter 10. Retina | Vaughan & Asbury's General Ophthalmology, 18e | AccessMedicine | McGraw-Hill Medical". accessmedicine.mhmedical.com. Retrieved 2017-03-07.
- "Diabetic Retinopathy | National Eye Institute". nei.nih.gov. Retrieved 2017-03-07.
- Hartnett, Mary Elizabeth; Cotten, C. Michael (2015). "Genomics in the neonatal nursery: Focus on ROP". Seminars in Perinatology. 39 (8): 604–610. doi:10.1053/j.semperi.2015.09.007. PMC 4644692. PMID 26477493.
- Zhang, Yun; Xia, Wei; Lu, Ping; Yuan, Huijuan (2016-11-06). "The Association between VDR Gene Polymorphisms and Diabetic Retinopathy Susceptibility: A Systematic Review and Meta-Analysis". BioMed Research International. 2016: 5305282. doi:10.1155/2016/5305282. ISSN 2314-6133. PMC 5116338. PMID 27891515.
- "Diabetic retinopathy: Screening". www.uptodate.com. Retrieved 2017-03-07.
- "Remote Retinal Screening Facilitates Diagnosis and Treatment of Retinopathy for Poor and/or Uninsured Patients With Diabetes in Rural California". Agency for Healthcare Research and Quality. 2013-10-03. Retrieved 2013-08-01.
- "Telemedicine-Based Eye Examinations Enhance Access, Reduce Costs, and Increase Satisfaction for Low-Income and Minority Patients with Diabetes". Agency for Healthcare Research and Quality. 2013-07-17. Retrieved 2013-08-01.
- Evans, J. R.; Michelessi, M.; Virgili, G. (2014). "Laser photocoagulation for proliferative diabetic retinopathy | Cochrane". The Cochrane Database of Systematic Reviews (11): CD011234. doi:10.1002/14651858.CD011234.pub2. PMC 6823265. PMID 25420029.
- Myint, K. T.; Sahoo, S.; Thein, A. W.; Moe, S.; Ni, H. (2015). "Laser therapy for retinopathy in sickle cell disease | Cochrane". The Cochrane Database of Systematic Reviews (10): CD010790. doi:10.1002/14651858.CD010790.pub2. PMID 26451693.
- Sankar, Mari Jeeva; Sankar, Jhuma; Chandra, Parijat (8 January 2018). "Anti-vascular endothelial growth factor (VEGF) drugs for treatment of retinopathy of prematurity". The Cochrane Database of Systematic Reviews. 1: CD009734. doi:10.1002/14651858.CD009734.pub3. ISSN 1469-493X. PMC 6491066. PMID 29308602.
- Martinez-Zapata, M. J.; Martí-Carvajal, A. J.; Solà, I.; Pijoán, J. I.; Buil-Calvo, J. A.; Cordero, J. A.; Evans, J. R. (2014). "Injections of anti-vascular endothelial growth factor for advanced diabetic retinopathy | Cochrane". The Cochrane Database of Systematic Reviews (11): CD008721. doi:10.1002/14651858.CD008721.pub2. PMC 6995643. PMID 25418485.
- "Retinopathy of Prematurity – Europe". American Academy of Ophthalmology. 2013-11-07. Retrieved 2017-03-03.
- "Retinal Physician -". www.retinalphysician.com. Retrieved 2017-03-03.
External links
| Classification |
|---|