Koch's postulates
Koch's postulates (/ˈkɔːx/)[2] are four criteria designed to establish a causative relationship between a microbe and a disease. The postulates were formulated by Robert Koch and Friedrich Loeffler in 1884, based on earlier concepts described by Jakob Henle,[3] and refined and published by Koch in 1890. Koch applied the postulates to describe the etiology of cholera and tuberculosis, but they have been controversially generalized to other diseases. These postulates were generated before modern concepts in microbial pathogenesis that cannot be examined using Koch's postulates, including viruses (which are obligate cellular parasites) and asymptomatic carriers. They have largely been supplanted by other criteria such as the Bradford Hill criteria for infectious disease causality in modern public health.

The postulates
Koch's postulates are the following:
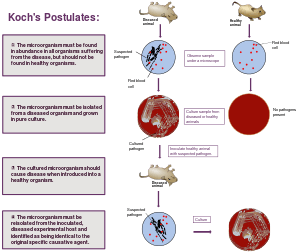
- The microorganism must be found in abundance in all organisms suffering from the disease, but should not be found in healthy organisms.
- The microorganism must be isolated from a diseased organism and grown in pure culture.
- The cultured microorganism should cause disease when introduced into a healthy organism.
- The microorganism must be reisolated from the inoculated, diseased experimental host and identified as being identical to the original specific causative agent.
However, Koch later abandoned the universalist requirement of the first postulate altogether when he discovered asymptomatic carriers of cholera[4] and, later, of typhoid fever. Asymptomatic or subclinical infection carriers are now known to be a common feature of many infectious diseases, especially viral diseases such as polio, herpes simplex, HIV/AIDS, and hepatitis C. As a specific example, all doctors and virologists agree that poliovirus causes paralysis in just a few infected subjects, and the success of the polio vaccine in preventing disease supports the conviction that the poliovirus is the causative agent.
The second postulate may also be suspended for certain microorganisms or entities that cannot (at the present time) be grown in pure culture.[5] Viruses also require host cells to grow and reproduce and therefore cannot be grown in pure cultures.
The third postulate specifies "should" not "must" because, as Koch himself proved in regard to both tuberculosis and cholera,[6] not all organisms exposed to an infectious agent will acquire the infection. Noninfection may be due to such factors as general health and proper immune functioning; acquired immunity from previous exposure or vaccination; or genetic immunity, as with the resistance to malaria conferred by possessing at least one sickle cell allele.
There are a few other exceptions to Koch's postulates. A single pathogen can cause several disease conditions. Additionally, a single disease condition can be caused by several different microorganisms. Some pathogens cannot be cultured in the lab, and some pathogens only cause disease in humans.[7]
In summary, an infectious agent that satisfies Koch's postulates can be concluded to cause disease, but the postulates' shortcomings mean they are not strictly necessary for this conclusion.
History
Koch's postulates were developed in the 19th century as general guidelines to identify pathogens that could be isolated with the techniques of the day.[8] Even in Koch's time, it was recognized that some infectious agents were clearly responsible for disease even though they did not fulfill all of the postulates.[4][6] Attempts to apply Koch's postulates rigidly to the diagnosis of viral diseases in the late 19th century, at a time when viruses could not be seen or isolated in culture, may have impeded the early development of the field of virology.[9][10] Koch's postulates have been recognized as largely obsolete by epidemiologists since the 1950s,[11][12] so, while retaining historical importance and continuing to inform the approach to microbiologic diagnosis, they are not routinely used to demonstrate causality.
Koch's postulates have also influenced scientists who examine microbial pathogenesis from a molecular point of view. In the 1980s, a molecular version of Koch's postulates was developed to guide the identification of microbial genes encoding virulence factors.[13]
That HIV causes AIDS does not follow from Koch's postulates,[14] which may have supported HIV/AIDS denialism. The role of oncoviruses in causing some cancers also does not follow Koch's postulates.[15]
While Koch's postulates have served the microbiology community well for nearly two centuries, new discoveries of methods of infections as a result of Koch and many others' work have shown that some diseases and conditions are not always caused by a single microbe species. According to a study by Oliver A. Todd and Brain M Peters, a newly discovered interaction between the pathogen Staphylococcus aureus and "fungal opportunist" Candida albicans is being considered a co-infection that is found in the bodies of sick patients who suffer from different conditions [2019]. This kind of synergism was found to be lethal in a separate study conducted by Carlson on mice. When mice were infected with the two pathogens independently, sickness resulted but the mice were able to recover. When infected with both pathogens together, the mice had a near-100% mortality rate, showing that some pathogens cannot be as easily isolated or may need extra techniques and steps that better prove causation of the disease.[16]
For the 21st century
Koch's postulates have played an important role in microbiology, yet they have major limitations. For example, Koch was well aware in the case of cholera that the causal agent, Vibrio cholerae, could be found in both sick and healthy people, invalidating his first postulate. Furthermore, viral diseases were not yet discovered when Koch formulated his postulates, and there are many viruses that do not cause illness in all infected individuals, a requirement of the first postulate. Additionally, it was known through experimentation that Helicobacter pylori caused mild inflammation of the gastric lining when ingested. As evident as the inflammation was, it still did not immediately convince skeptics that H. pylori was associated with ulcers. Eventually, skeptics were silenced when a newly developed antibiotic treatment eliminated the bacteria and ultimately cured the disease. Koch's postulates are also of limited effectiveness when evaluating biofilms, Somni cells, and viruses. Cultivation of biofilms requires cultivation by molecular methods rather than traditional methods, and these alternative methods do not detect the cause of infection, which therefore interferes with the third postulate, that microorganisms should cause disease.[17] Somni cells and viruses cannot be cultured. The Somni cells, also called sleeping cells, become dormant due to strain on the cell. This state of sleep prevents the cell from growing in the culture.[18] This is similar to how viruses cannot grow in axenic culture: viruses must be living to replicate, so the culture is not a suitable host.[19] Allyson Byrd and Julia Segre have proposed changes to the postulates to make them more accurate for today's world. Their revisions involve the third postulate: they disagree that a pathogen will always cause disease. Their first revision involves colonization resistance. Colonization resistance allows an organism to feed off of the host and protect it from pathogens that would have caused disease if the organism was not attached to the host. Their second revision is that a community of microbes could help inhibit pathogens even further, preventing the pathogen from spreading disease as it is supposed to.[20] Similar to Byrd and Segre, Thomas Rivers suggested revisions to Koch's postulates. He believed that, although the original postulates were made as a guide, they were actually an obstacle. Rivers wanted to show the link between viruses and diseases. Rivers cultivated his own postulates; the first stated that the virus must be connected to disease consistently. Secondly, the outcome of experimentation must indicate that the virus is directly responsible for the disease.[21] Contradictions and occurrences such as these have led many to believe that a fifth postulate may be required. If enacted, this postulate would state that sufficient microbial data should allow scientists to treat, cure, or prevent the particular disease.
More recently, modern nucleic-acid-based microbial detection methods have made Koch's original postulates even less relevant. These methods enable the identification of microbes that are associated with a disease, but which cannot be cultured. Also, these methods are very sensitive, and can often detect very low levels of viruses in healthy people.
These new methods have led to revised versions of Koch's postulates. Fredricks and Relman have suggested the following postulates for the 21st century:[22]
- A nucleic acid sequence belonging to a putative pathogen should be present in most cases of an infectious disease. Microbial nucleic acids should be found preferentially in those organs or gross anatomic sites known to be diseased, and not in those organs that lack pathology.
- Fewer, or no, copies of pathogen-associated nucleic acid sequences should occur in hosts or tissues without disease.
- With resolution of disease, the copy number of pathogen-associated nucleic acid sequences should decrease or become undetectable. With clinical relapse, the opposite should occur.
- When sequence detection predates disease, or sequence copy number correlates with severity of disease or pathology, the sequence-disease association is more likely to be a causal relationship.
- The nature of the microorganism inferred from the available sequence should be consistent with the known biological characteristics of that group of organisms.
- Tissue-sequence correlates should be sought at the cellular level: efforts should be made to demonstrate specific in situ hybridization of microbial sequence to areas of tissue pathology and to visible microorganisms or to areas where microorganisms are presumed to be located.
- These sequence-based forms of evidence for microbial causation should be reproducible.
These modifications are still controversial in that they do not account well for established disease associations, such as papillomavirus and cervical cancer, nor do they take into account prion diseases, which have no nucleic acid sequences of their own.
See also
References
- Koch, R. (1876). "Untersuchungen über Bakterien: V. Die Ätiologie der Milzbrand-Krankheit, begründet auf die Entwicklungsgeschichte des Bacillus anthracis" [Investigations into bacteria: V. The etiology of anthrax, based on the ontogenesis of Bacillus anthracis] (PDF). Cohns Beitrage zur Biologie der Pflanzen (in German). 2 (2): 277–310.
- "Koch". Random House Webster's Unabridged Dictionary.
- Evans AS (October 1978). "Causation and disease: a chronological journey. The Thomas Parran Lecture". American Journal of Epidemiology. 108 (4): 249–58. doi:10.1093/oxfordjournals.aje.a112617. PMID 727194.
- Koch, R. (1893). "Ueber den augenblicklichen Stand der bakteriologischen Choleradiagnose" [About the instantaneous state of the bacteriological diagnosis of cholera]. Zeitschrift für Hygiene und Infektionskrankheiten (in German). 14: 319–38. doi:10.1007/BF02284324.
- Inglis TJ (November 2007). "Principia aetiologica: taking causality beyond Koch's postulates". Journal of Medical Microbiology. 56 (Pt 11): 1419–22. doi:10.1099/jmm.0.47179-0. PMID 17965339. Archived from the original on 2010-03-05. Retrieved 2010-07-20.
- Koch Robert (1884). "2 Die Aetiologie der Tuberkulose". Mitt Kaiser Gesundh. pp. 1–88.
- Slonczewski, Joan; Foster, John (2011). Microbiology An Evolving Science Second Edition. New York, N.Y.: W. W. Norton & Company, Inc. pp. 20–22. ISBN 978-0-393-93447-2.
- Walker L, Levine H, Jucker M (2006). "Koch's postulates and infectious proteins". Acta Neuropathol. 112 (1): 1–4. doi:10.1007/s00401-006-0072-x. PMID 16703338.
- Brock TD (1999). Robert Koch: a life in medicine and bacteriology. Washington DC: American Society of Microbiology Press. ISBN 1-55581-143-4.
- Evans AS (May 1976). "Causation and disease: the Henle-Koch postulates revisited". Yale J Biol Med. 49 (2): 175–95. PMC 2595276. PMID 782050.
- Huebner, Robert J. (April 1957). "Criteria for etiologic association of prevalent viruses with prevalent diseases; the virologist's dilemma". Annals of the New York Academy of Sciences. 67 (8): 430–8. Bibcode:1957NYASA..67..430H. doi:10.1111/j.1749-6632.1957.tb46066.x. PMID 13411978.
- Evans AS (December 1995). "Causation and disease: a chronological journey. The Thomas Parran Lecture. 1978". American Journal of Epidemiology. 142 (11): 1126–35, discussion 1125. doi:10.1093/oxfordjournals.aje.a117571. PMID 7485059.
- Falkow S (1988). "Molecular Koch's postulates applied to microbial pathogenicity". Rev. Infect. Dis. 10 (Suppl 2): S274–6. doi:10.1093/cid/10.Supplement_2.S274. PMID 3055197.
- Weiss, Robin A.; Jaffe, Harold W. (1990). "Duesberg, HIV and AIDS". Nature. 345 (6277): 659–60. Bibcode:1990Natur.345..659W. doi:10.1038/345659a0. PMID 2163025.
- Moore, Patrick S.; Chang, Yuan (2013). "The conundrum of causality in tumor virology: The cases of KSHV and MCV". Seminars in Cancer Biology. 26: 4–12. doi:10.1016/j.semcancer.2013.11.001. PMC 4040341. PMID 24304907.
- Todd, Olivia; Peters, Brian (3 September 2019). "Candida Albicans and Staphylococcus aureus Pathogenicity and Polymicrobial Interactions: Lessons beyond Koch's Postulates". Journal of Fungi. 5 (81).
- Hosainzadegan, Hasan; Rovshan, Khalilov; Gholizadeh, Pourya (12 August 2019). "The necessity to revise Koch's postulates and its application to infectious and non-infectious diseases: a mini-review". European Journal of Clinical Microbiology & Infectious Diseases: 4. doi:10.1007/s10096-019-03681-1. PMID 31440916.
- Grimes, Jay (1 May 2006). "Koch's Postulates - Then and Now" (PDF). American Society for Microbiology. 1: 226. Retrieved 4 October 2019.
- Fredricks, David; Relman, David (January 1996). "Sequence-Based Identification of Microbial Pathogens: a Reconsideration of Koch's Postulates" (PDF). Clinical Microbiology Reviews. 9 (1): 20–21. doi:10.1128/CMR.9.1.18. PMC 172879. PMID 8665474. Retrieved October 7, 2019.
- Byrd, Allyson; Segre, Julia (15 January 2016). "Adapting Koch's Postulates". Science. 351 (6270): 224–226. doi:10.1126/science.aad6753. PMID 26816362. Retrieved October 7, 2019.
- Fredricks, David; Relman, David (January 1996). "Sequence-Based Identification of Microbial Pathogens: a Reconsideration of Koch's Postulates" (PDF). Clinical Microbiology Reviews. 9 (1): 20–21. doi:10.1128/CMR.9.1.18. PMC 172879. PMID 8665474. Retrieved October 7, 2019.
- Fredericks DN, Relman DA (1996). "Sequence-based identification of microbial pathogens: a reconsideration of Koch's postulates". Clin Microbiol Rev. 9 (1): 18–33. doi:10.1128/CMR.9.1.18. PMC 172879. PMID 8665474.
Further reading
- Contagion: Historical Views of Diseases and Epidemics from Harvard Library