Thrombophilia
Thrombophilia (sometimes called hypercoagulability or a prothrombotic state) is an abnormality of blood coagulation that increases the risk of thrombosis (blood clots in blood vessels).[1][2] Such abnormalities can be identified in 50% of people who have an episode of thrombosis (such as deep vein thrombosis in the leg) that was not provoked by other causes.[3] A significant proportion of the population has a detectable thrombophilic abnormality, but most of these develop thrombosis only in the presence of an additional risk factor.[2]
| Thrombophilia | |
|---|---|
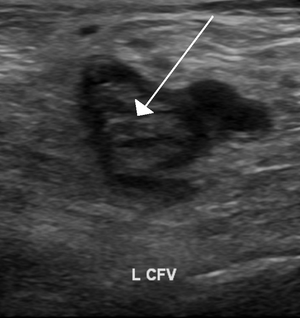 | |
| An ultrasound image demonstrating a blood clot in the left common femoral vein. | |
| Specialty | Hematology |

There is no specific treatment for most thrombophilias, but recurrent episodes of thrombosis may be an indication for long-term preventive anticoagulation.[2] The first major form of thrombophilia to be identified by medical science, antithrombin deficiency, was identified in 1965, while the most common abnormalities (including factor V Leiden) were described in the 1990s.[4][5]
Signs and symptoms

The most common conditions associated with thrombophilia are deep vein thrombosis (DVT) and pulmonary embolism (PE), which are referred to collectively as venous thromboembolism (VTE). DVT usually occurs in the legs, and is characterized by pain, swelling and redness of the limb. It may lead to long-term swelling and heaviness due to damage to valves in the veins.[6] The clot may also break off and migrate (embolize) to arteries in the lungs. Depending on the size and the location of the clot, this may lead to sudden-onset shortness of breath, chest pain, palpitations and may be complicated by collapse, shock and cardiac arrest.[2][7]
Venous thrombosis may also occur in more unusual places: in the veins of the brain, liver (portal vein thrombosis and hepatic vein thrombosis), mesenteric vein, kidney (renal vein thrombosis) and the veins of the arms.[2] Whether thrombophilia also increases the risk of arterial thrombosis (which is the underlying cause of heart attacks and strokes) is less well established.[2][8][9]
Thrombophilia has been linked to recurrent miscarriage,[10] and possibly various complications of pregnancy such as intrauterine growth restriction, stillbirth, severe pre-eclampsia and abruptio placentae.[2]
Protein C deficiency may cause purpura fulminans, a severe clotting disorder in the newborn that leads to both tissue death and bleeding into the skin and other organs. The condition has also been described in adults. Protein C and protein S deficiency have also been associated with an increased risk of skin necrosis on commencing anticoagulant treatment with warfarin or related drugs.[2][11]
Causes
Thrombophilia can be congenital or acquired. Congenital thrombophilia refers to inborn conditions (and usually hereditary, in which case "hereditary thrombophilia" may be used) that increase the tendency to develop thrombosis, while, on the other hand, acquired thrombophilia refers to conditions that arise later in life.
Congenital
The most common types of congenital thrombophilia are those that arise as a result of overactivity of coagulation factors. They are relatively mild, and are therefore classified as "type II" defects.[12] The most common ones are factor V Leiden (a mutation in the F5 gene at position 1691) and prothrombin G20210A, a mutation in prothrombin (at position 20210 in the 3' untranslated region of the gene).[1][13]
The rare forms of congenital thrombophilia are typically caused by a deficiency of natural anticoagulants. They are classified as "type I" and are more severe in their propensity to cause thrombosis.[12] The main ones are antithrombin III deficiency, protein C deficiency and protein S deficiency.[1][13] Milder rare congenital thrombophilias are factor XIII mutation[13] and familial dysfibrinogenemia (an abnormal fibrinogen).[13] It is unclear whether congenital disorders of fibrinolysis (the system that destroys clots) are major contributors to thrombosis risk.[12] Congenital deficiency of plasminogen, for instance, mainly causes eye symptoms and sometimes problems in other organs, but the link with thrombosis has been more uncertain.[14]
Blood group determines thrombosis risk to a significant extent. Those with blood groups other than type O are at a two- to fourfold relative risk. O blood group is associated with reduced levels of von Willebrand factor – because of increased clearance – and factor VIII, which is related to thrombotic risk .[5]
Acquired
A number of acquired conditions augment the risk of thrombosis. A prominent example is antiphospholipid syndrome,[1][13] which is caused by antibodies against constituents of the cell membrane, particularly lupus anticoagulant (first found in people with the disease systemic lupus erythematosus but often detected in people without the disease), anti-cardiolipin antibodies, and anti-β2-glycoprotein 1 antibodies; it is therefore regarded as an autoimmune disease. In some cases antiphospholipid syndrome can cause arterial as well as venous thrombosis. It is also more strongly associated with miscarriage, and can cause a number of other symptoms (such as livedo reticularis of the skin and migraine).[15]
Heparin-induced thrombocytopenia (HIT) is due to an immune system reaction against the anticoagulant drug heparin (or its derivatives).[1] Though it is named for associated low platelet counts, HIT is strongly associated with risk of venous and arterial thrombosis.[16] Paroxysmal nocturnal hemoglobinuria (PNH) is a rare condition resulting from acquired alterations in the PIGA gene, which plays a role in the protection of blood cells from the complement system. PNH increases the risk of venous thrombosis but is also associated with hemolytic anemia (anemia resulting from destruction of red blood cells).[17] Both HIT and PNH require particular treatment.[16][17]
Hematologic conditions associated with sluggish blood flow can increase risk for thrombosis. For example, sickle-cell disease (caused by mutations of hemoglobin) is regarded as a mild prothrombotic state induced by impaired flow.[1] Similarly, myeloproliferative disorders, in which the bone marrow produces too many blood cells, predispose to thrombosis, particularly in polycythemia vera (excess red blood cells) and essential thrombocytosis (excess platelets). Again, these conditions usually warrant specific treatment when identified.[18]
Cancer, particularly when metastatic (spread to other places in the body), is a recognised risk factor for thrombosis.[2][13] A number of mechanisms have been proposed, such as activation of the coagulation system by cancer cells or secretion of procoagulant substances. Furthermore, particular cancer treatments (such as the use of central venous catheters for chemotherapy) may increase the risk of thrombosis further.[19]
Nephrotic syndrome, in which protein from the bloodstream is released into the urine due to kidney diseases, can predispose to thrombosis;[1] this is particularly the case in more severe cases (as indicated by blood levels of albumin below 25 g/l) and if the syndrome is caused by the condition membranous nephropathy.[20] Inflammatory bowel disease (ulcerative colitis and Crohn's disease) predispose to thrombosis, particularly when the disease is active. Various mechanisms have been proposed.[2][21]
Pregnancy is associated with an increased risk of thrombosis. This probably results from a physiological hypercoagulability in pregnancy that protects against postpartum hemorrhage.[22]
The female hormone estrogen, when used in the combined oral contraceptive pill and in perimenopausal hormone replacement therapy, has been associated with a two- to sixfold increased risk of venous thrombosis. The risk depends on the type of hormones used, the dose of estrogen, and the presence of other thrombophilic risk factors.[23] Various mechanisms, such as deficiency of protein S and tissue factor pathway inhibitor, are said to be responsible.[24]
Obesity has long been regarded as a risk factor for venous thrombosis. It more than doubles the risk in numerous studies, particularly in combination with the use of oral contraceptives or in the period after surgery. Various coagulation abnormalities have been described in the obese. Plasminogen activator inhibitor-1, an inhibitor of fibrinolysis, is present in higher levels in people with obesity. Obese people also have larger numbers of circulating microvesicles (fragments of damaged cells) that bear tissue factor. Platelet aggregation may be increased, and there are higher levels of coagulation proteins such as von Willebrand factor, fibrinogen, factor VII and factor VIII. Obesity also increases the risk of recurrence after an initial episode of thrombosis.[25]
Unclear
A number of conditions that have been linked with venous thrombosis are possibly genetic and possibly acquired.[13] These include: elevated levels of factor VIII, factor IX, factor XI, fibrinogen and thrombin-activatable fibrinolysis inhibitor, and decreased levels of tissue factor pathway inhibitor. Activated protein C resistance that is not attributable to factor V mutations is probably caused by other factors and remains a risk factor for thrombosis.[13]
There is an association between the blood levels of homocysteine and thrombosis,[13] although this has not been reported consistently in all studies.[5] Homocysteine levels are determined by mutations in the MTHFR and CBS genes, but also by levels of folic acid, vitamin B6 and vitamin B12, which depend on diet.[12]
Mechanism
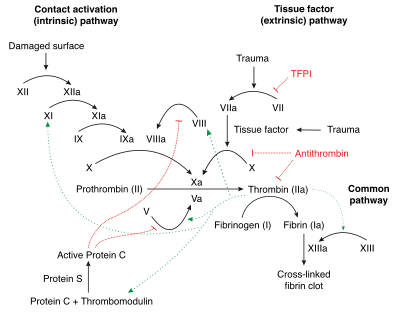
Thrombosis is a multifactorial problem because there are often multiple reasons why a person might develop thrombosis. These risk factors may include any combination of abnormalities in the blood vessel wall, abnormalities in the blood flow (as in immobilization), and abnormalities in the consistency of the blood. Thrombophilia is caused by abnormalities in blood consistency, which is determined by the levels of coagulation factors and other circulating blood proteins that participate in the "coagulation cascade".[13]
Normal coagulation is initiated by the release of tissue factor from damaged tissue. Tissue factor binds to circulating factor VIIa. The combination activates factor X to factor Xa and factor IX to factor IXa. Factor Xa (in the presence of factor V) activates prothrombin into thrombin. Thrombin is a central enzyme in the coagulation process: it generates fibrin from fibrinogen, and activates a number of other enzymes and cofactors (factor XIII, factor XI, factor V and factor VIII, TAFI) that enhance the fibrin clot.[12] The process is inhibited by TFPI (which inactivates the first step catalyzed by factor VIIa/tissue factor), antithrombin (which inactivates thrombin, factor IXa, Xa and XIa), protein C (which inhibits factors Va and VIIIa in the presence of protein S), and protein Z (which inhibits factor Xa).[12]
In thrombophilia, the balance between "procoagulant" and "anticoagulant" activity is disturbed. The severity of the imbalance determines the likelihood that someone develops thrombosis. Even small perturbances of proteins, such as the reduction of antithrombin to only 70–80% of the normal level, can increase the thrombosis risk; this is in contrast with hemophilia, which only arises if levels of coagulation factors are markedly decreased.[12]
In addition to its effects on thrombosis, hypercoagulable states may accelerate the development of atherosclerosis, the arterial disease that underlies myocardial infarction and other forms of cardiovascular disease.[26][27]
Diagnosis
Tests for thrombophilia include complete blood count (with examination of the blood film), prothrombin time, partial thromboplastin time, thrombodynamics test, thrombin time and reptilase time, lupus anticoagulant, anti-cardiolipin antibody, anti-β2 glycoprotein 1 antibody, activated protein C resistance, fibrinogen tests, factor V Leiden and prothrombin mutation, and basal homocysteine levels.[2] Testing may be more or less extensive depending on clinical judgement and abnormalities detected on initial evaluation.[2]
For hereditary cases, the patient must have at least two abnormal tests plus family history.
Screening
There are divergent views as to whether everyone with an unprovoked episode of thrombosis should be investigated for thrombophilia. Even those with a form of thrombophilia may not necessarily be at risk of further thrombosis, while recurrent thrombosis is more likely in those who have had previous thrombosis even in those who have no detectable thrombophilic abnormalities.[8][11][28] Recurrent thromboembolism, or thrombosis in unusual sites (e.g. the hepatic vein in Budd-Chiari syndrome), is a generally accepted indication for screening. It is more likely to be cost-effective in people with a strong personal or family history of thrombosis.[29] In contrast, the combination of thrombophilia with other risk factors may provide an indication for preventive treatment, which is why thrombophilia testing may be performed even in those who would not meet the strict criteria for these tests.[28] Searching for a coagulation abnormality is not normally undertaken in patients in whom thrombosis has an obvious trigger. For example, if the thrombosis is due to immobilization after recent orthopedic surgery, it is regarded as "provoked" by the immobilization and the surgery and it is less likely that investigations will yield clinically important results.[11][28]
When venous thromboembolism occurs when a patient is experiencing transient major risk factors such as prolonged immobility, surgery, or trauma, testing for thrombophilia is not appropriate because the outcome of the test would not change a patient's indicated treatment.[30][31] In 2013, the American Society of Hematology, as part of recommendations in the Choosing Wisely campaign, cautioned against overuse of thrombophilia screening; false positive results of testing would lead to people inappropriately being labeled as having thrombophilia, and being treated with anticoagulants without clinical need[30]
In the United Kingdom, professional guidelines give specific indications for thrombophilia testing. It is recommended that testing be done only after appropriate counseling, and hence the investigations are usually not performed at the time when thrombosis is diagnosed but at a later time.[11] In particular situations, such as retinal vein thrombosis, testing is discouraged altogether because thrombophilia is not regarded as a major risk factor. In other rare conditions generally linked with hypercoagulability, such as cerebral venous thrombosis and portal vein thrombosis, there is insufficient data to state for certain whether thrombophilia screening is helpful, and decisions on thrombophilia screening in these conditions are therefore not regarded as evidence-based.[11] If cost-effectiveness (quality-adjusted life years in return for expenditure) is taken as a guide, it is generally unclear whether thrombophilia investigations justify the often high cost,[32] unless the testing is restricted to selected situations.[33]
Recurrent miscarriage is an indication for thrombophilia screening, particularly antiphospholipid antibodies (anti-cardiolipin IgG and IgM, as well as lupus anticoagulant), factor V Leiden and prothrombin mutation, activated protein C resistance and a general assessment of coagulation through an investigation known as thromboelastography.[10]
Women who are planning to use oral contraceptives do not benefit from routine screening for thrombophilias, as the absolute risk of thrombotic events is low. If either the woman or a first-degree relative has suffered from thrombosis, the risk of developing thrombosis is increased. Screening this selected group may be beneficial,[24] but even when negative may still indicate residual risk.[11] Professional guidelines therefore suggest that alternative forms of contraception be used rather than relying on screening.[11]
Thrombophilia screening in people with arterial thrombosis is generally regarded unrewarding and is generally discouraged,[11] except possibly for unusually young patients (especially when precipitated by smoking or use of estrogen-containing hormonal contraceptives) and those in whom revascularization, such as coronary arterial bypass, fails because of rapid occlusion of the graft.[9]
Treatment

There is no specific treatment for thrombophilia, unless it is caused by an underlying medical illness (such as nephrotic syndrome), where the treatment of the underlying disease is needed. In those with unprovoked and/or recurrent thrombosis, or those with a high-risk form of thrombophilia, the most important decision is whether to use anticoagulation medications, such as warfarin, on a long-term basis to reduce the risk of further episodes.[3] This risk needs to weighed against the risk that the treatment will cause significant bleeding, as the reported risk of major bleeding is over 3% per year, and 11% of those with major bleeding may die as a result.[3]
Apart from the abovementioned forms of thrombophilia, the risk of recurrence after an episode of thrombosis is determined by factors such as the extent and severity of the original thrombosis, whether it was provoked (such as by immobilization or pregnancy), the number of previous thrombotic events, male sex, the presence of an inferior vena cava filter, the presence of cancer, symptoms of post-thrombotic syndrome, and obesity.[3] These factors tend to be more important in the decision than the presence or absence of a detectable thrombophilia.[11][34]
Those with antiphospholipid syndrome may be offered long-term anticoagulation after a first unprovoked episode of thrombosis. The risk is determined by the subtype of antibody detected, by the antibody titer (amount of antibodies), whether multiple antibodies are detected, and whether it is detected repeatedly or only on a single occasion.[15]
Women with a thrombophilia who are contemplating pregnancy or are pregnant usually require alternatives to warfarin during pregnancy, especially in the first 13 weeks, when it may produce abnormalities in the unborn child. Low molecular weight heparin (LMWH, such as enoxaparin) is generally used as an alternative.[35] Warfarin and LMWH may safely be used in breastfeeding.[35]
When women experience recurrent pregnancy loss secondary to thrombophilia, some studies have suggested that low molecular weight heparin reduces the risk of miscarriage. When the results of all studies are analysed together, no statistically significant benefit could be demonstrated.[36]
Prognosis
In people without a detectable thrombophilia, the cumulative risk of developing thrombosis by the age of 60 is about 12%. About 60% of people who are deficient in antithrombin will have experienced thrombosis at least once by age 60, as will about 50% of people with protein C deficiency and about a third of those with protein S deficiency. People with activated protein C resistance (usually resulting from factor V Leiden), in contrast, have a slightly raised absolute risk of thrombosis, with 15% having had at least one thrombotic event by the age of sixty.[12] In general, men are more likely than women to experience repeated episodes of venous thrombosis.[5]
People with factor V Leiden are at a relatively low risk of thrombosis, but may develop thrombosis in the presence of an additional risk factor, such as immobilization. Most people with the prothrombin mutation (G20210A) never develop thrombosis.[12]
Epidemiology
The major ("type 1") thrombophilias are rare. Antithrombin deficiency is present in 0.2% of the general population and 0.5–7.5% of people with venous thrombosis. Protein C deficiency, too, is present in 0.2% of the population, and can be found in 2.5–6% of people with thrombosis. The exact prevalence of protein S deficiency in the population is unknown; it is found 1.3–5% of people with thrombosis.[12]
The minor ("type 2") thrombophilias are much more common. Factor V Leiden is present in 5% of the population of Northern European descent, but much rarer in those of Asian or African extraction. In people with thrombosis, 10% have factor V Leiden. In those who are referred for thrombophilia testing, 30–50% have the defect. The prothrombin mutation occurs at rates of 1–4% in the general population, 5–10% of people with thrombosis, and 15% of people referred for thrombophilia testing. Like factor V Leiden, this abnormality is uncommon in Africans and Asians.[12]
The exact prevalence of antiphospholipid syndrome is not well known, as different studies employ different definitions of the condition. Antiphospholipid antibodies are detected in 24% of those referred to thrombophilia testing.[15]
History

German physician Rudolf Virchow categorized abnormalities in the consistency of the blood as a factor in the development of thrombosis in 1856. The exact nature of these abnormalities remained elusive until the first form of thrombophilia, antithrombin deficiency, was recognized in 1965 by the Norwegian hematologist Olav Egeberg.[37] Protein C deficiency followed in 1981, when described by researchers from the Scripps Research Institute and the U.S. Centers of Disease Control.[38] Protein S deficiency followed in 1984, described by researchers at the University of Oklahoma.[4][5][39]
Antiphospholipid syndrome was described in full in the 1980s, after various previous reports of specific antibodies in people with systemic lupus erythematosus and thrombosis.[15][40] The syndrome is often attributed to the British rheumatologist Graham R.V. Hughes, and is often referred to as Hughes syndrome for that reason.[41]
The more common genetic thrombophilias were described in the 1990s. Many studies had previously indicated that many people with thrombosis showed resistance activated protein C. In 1994 a group in Leiden, The Netherlands, identified the most common underlying defect—a mutation in factor V that made it resistant to the action of activated protein C. The defect was called factor V Leiden, as genetic abnormalities are typically named after the place where they are discovered.[42] Two years later, the same group described a common mutation in the prothrombin gene that caused elevation of prothrombin levels and a mild increase in thrombosis risk.[4][5][43]
It is suspected that other genetic abnormalities underlying familial thrombosis will in future be discovered through studies of the entire genetic code, looking for small alternations in genes.[4][5]
References
- Mitchell RS, Kumar V, Abbas AK, Fausto N (2007). "Chapter 4". Robbins Basic Pathology (Eighth ed.). Philadelphia: Saunders. ISBN 978-1-4160-2973-1.
- Heit JA (2007). "Thrombophilia: common questions on laboratory assessment and management". Hematology Am. Soc. Hematol. Educ. Program. 2007 (1): 127–35. doi:10.1182/asheducation-2007.1.127. PMID 18024620.
- Kyrle PA, Rosendaal FR, Eichinger S (December 2010). "Risk assessment for recurrent venous thrombosis". Lancet. 376 (9757): 2032–9. doi:10.1016/S0140-6736(10)60962-2. PMID 21131039. S2CID 31610364.
- Dahlbäck B (July 2008). "Advances in understanding pathogenic mechanisms of thrombophilic disorders". Blood. 112 (1): 19–27. doi:10.1182/blood-2008-01-077909. PMID 18574041.
- Rosendaal FR, Reitsma PH (July 2009). "Genetics of venous thrombosis". J. Thromb. Haemost. 7 Suppl 1: 301–4. doi:10.1111/j.1538-7836.2009.03394.x. PMID 19630821.
- Scarvelis D, Wells PS (October 2006). "Diagnosis and treatment of deep-vein thrombosis". CMAJ. 175 (9): 1087–92. doi:10.1503/cmaj.060366. PMC 1609160. PMID 17060659.
- Agnelli G, Becattini C (July 2010). "Acute pulmonary embolism". N. Engl. J. Med. 363 (3): 266–74. doi:10.1056/NEJMra0907731. PMID 20592294.
- Middeldorp S, van Hylckama Vlieg A (August 2008). "Does thrombophilia testing help in the clinical management of patients?". Br. J. Haematol. 143 (3): 321–35. doi:10.1111/j.1365-2141.2008.07339.x. PMID 18710381.
- de Moerloose P, Boehlen F (April 2007). "Inherited thrombophilia in arterial disease: a selective review". Semin. Hematol. 44 (2): 106–13. doi:10.1053/j.seminhematol.2007.01.008. PMID 17433903.
- Rai R, Regan L (August 2006). "Recurrent miscarriage". Lancet. 368 (9535): 601–11. doi:10.1016/S0140-6736(06)69204-0. PMID 16905025. S2CID 42968924.
- Baglin T, Gray E, Greaves M, et al. (April 2010). "Clinical guidelines for testing for heritable thrombophilia". Br. J. Haematol. 149 (2): 209–20. doi:10.1111/j.1365-2141.2009.08022.x. PMID 20128794.
- Crowther MA, Kelton JG (2003). "Congenital thrombophilic states associated with venous thrombosis: a qualitative overview and proposed classification system". Ann. Intern. Med. 138 (2): 128–34. doi:10.7326/0003-4819-138-2-200301210-00014. PMID 12529095. S2CID 43161448. Lay summary.
- Rosendaal FR (2005). "Venous thrombosis: the role of genes, environment, and behavior". Hematology Am. Soc. Hematol. Educ. Program. 2005 (1): 1–12. doi:10.1182/asheducation-2005.1.1. PMID 16304352.
- Mehta R, Shapiro AD (November 2008). "Plasminogen deficiency". Haemophilia. 14 (6): 1261–8. doi:10.1111/j.1365-2516.2008.01825.x. PMID 19141167.
- Ruiz-Irastorza G, Crowther M, Branch W, Khamashta MA (October 2010). "Antiphospholipid syndrome". Lancet. 376 (9751): 1498–509. doi:10.1016/S0140-6736(10)60709-X. hdl:2318/1609788. PMID 20822807. S2CID 25554663.
- Keeling D, Davidson S, Watson H (May 2006). "The management of heparin-induced thrombocytopenia". Br. J. Haematol. 133 (3): 259–69. doi:10.1111/j.1365-2141.2006.06018.x. PMID 16643427. Archived from the original on 2012-12-10.
- Brodsky RA (April 2008). "Narrative review: paroxysmal nocturnal hemoglobinuria: the physiology of complement-related hemolytic anemia". Ann. Intern. Med. 148 (8): 587–95. CiteSeerX 10.1.1.668.4942. doi:10.7326/0003-4819-148-8-200804150-00003. PMID 18413620. S2CID 19715590.
- Papadakis E, Hoffman R, Brenner B (November 2010). "Thrombohemorrhagic complications of myeloproliferative disorders". Blood Rev. 24 (6): 227–32. doi:10.1016/j.blre.2010.08.002. PMID 20817333.
- Prandoni P, Falanga A, Piccioli A (June 2005). "Cancer and venous thromboembolism". Lancet Oncol. 6 (6): 401–10. doi:10.1016/S1470-2045(05)70207-2. PMID 15925818.
- Hull RP, Goldsmith DJ (May 2008). "Nephrotic syndrome in adults". BMJ. 336 (7654): 1185–9. doi:10.1136/bmj.39576.709711.80. PMC 2394708. PMID 18497417.
- Quera R, Shanahan F (October 2004). "Thromboembolism--an important manifestation of inflammatory bowel disease". Am. J. Gastroenterol. 99 (10): 1971–3. PMID 15447758.
- Bourjeily G, Paidas M, Khalil H, Rosene-Montella K, Rodger M (February 2010). "Pulmonary embolism in pregnancy". Lancet. 375 (9713): 500–12. doi:10.1016/S0140-6736(09)60996-X. PMID 19889451. S2CID 8633455.
- Gomes MP, Deitcher SR (October 2004). "Risk of venous thromboembolic disease associated with hormonal contraceptives and hormone replacement therapy: a clinical review". Arch. Intern. Med. 164 (18): 1965–76. doi:10.1001/archinte.164.18.1965. PMID 15477430.
- Tchaikovski SN, Rosing J (July 2010). "Mechanisms of estrogen-induced venous thromboembolism". Thromb. Res. 126 (1): 5–11. doi:10.1016/j.thromres.2010.01.045. PMID 20163835.
- Stein PD, Goldman J (September 2009). "Obesity and thromboembolic disease". Clin. Chest Med. 30 (3): 489–93, viii. doi:10.1016/j.ccm.2009.05.006. PMID 19700047.
- Borissoff JI, Spronk HM, Heeneman S, ten Cate H (2009). "Is thrombin a key player in the 'coagulation-atherogenesis' maze?". Cardiovasc. Res. 82 (3): 392–403. doi:10.1093/cvr/cvp066. PMID 19228706.
- Borissoff JI, Spronk HM, ten Cate H (2011). "The hemostatic system as a modulator of atherosclerosis". N. Engl. J. Med. 364 (18): 1746–1760. doi:10.1056/NEJMra1011670. PMID 21542745.
- Dalen JE (June 2008). "Should patients with venous thromboembolism be screened for thrombophilia?". Am. J. Med. 121 (6): 458–63. doi:10.1016/j.amjmed.2007.10.042. PMID 18501222.
- Wu O, Robertson L, Twaddle S, et al. (October 2005). "Screening for thrombophilia in high-risk situations: a meta-analysis and cost-effectiveness analysis". Br. J. Haematol. 131 (1): 80–90. doi:10.1111/j.1365-2141.2005.05715.x. PMID 16173967.
- American Society of Hematology (September 2013), "Five Things Physicians and Patients Should Question", Choosing Wisely: an initiative of the ABIM Foundation, American Society of Hematology, retrieved 10 December 2013, which cites
- Chong, L. -Y.; Fenu, E.; Stansby, G.; Hodgkinson, S.; Guideline Development, G. (2012). "Management of venous thromboembolic diseases and the role of thrombophilia testing: Summary of NICE guidance". BMJ. 344: e3979. doi:10.1136/bmj.e3979. PMID 22740565. S2CID 42342532.
- Baglin, T.; Gray, E.; Greaves, M.; Hunt, B. J.; Keeling, D.; Machin, S.; MacKie, I.; Makris, M.; Nokes, T.; Perry, D.; Tait, R. C.; Walker, I.; Watson, H.; British Committee for Standards in Haematology (2010). "Clinical guidelines for testing for heritable thrombophilia". British Journal of Haematology. 149 (2): 209–220. doi:10.1111/j.1365-2141.2009.08022.x. PMID 20128794.
- Hicks LK, Bering H, Carson KR, et al. (2013). "The ASH Choosing Wisely(R) campaign: five hematologic tests and treatments to question". Blood. 122 (24): 3879–83. doi:10.1182/blood-2013-07-518423. PMID 24307720.
- Simpson EL, Stevenson MD, Rawdin A, Papaioannou D (January 2009). "Thrombophilia testing in people with venous thromboembolism: systematic review and cost-effectiveness analysis". Health Technol. Assess. 13 (2): iii, ix–x, 1–91. doi:10.3310/hta13020. PMID 19080721.
- Wu O, Greer IA (September 2007). "Is screening for thrombophilia cost-effective?". Curr. Opin. Hematol. 14 (5): 500–3. doi:10.1097/MOH.0b013e32825f5318. PMID 17934357. S2CID 22896788.
- Kearon C, Kahn SR, Agnelli G, Goldhaber S, Raskob GE, Comerota AJ (June 2008). "Antithrombotic therapy for venous thromboembolic disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition)". Chest. 133 (6 Suppl): 454S–545S. doi:10.1378/chest.08-0658. PMID 18574272. Archived from the original on 2013-01-12.
- Bates SM, Greer IA, Pabinger I, Sofaer S, Hirsh J (June 2008). "Venous thromboembolism, thrombophilia, antithrombotic therapy, and pregnancy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition)". Chest. 133 (6 Suppl): 844S–886S. doi:10.1378/chest.08-0761. PMID 18574280. Archived from the original on 2013-01-12.
- Skeith L, Carrier M, Kaaja R, Martinelli I, Petroff D, Schleußner E, Laskin CA, Rodger MA (2016). "A meta-analysis of low-molecular-weight heparin to prevent pregnancy loss in women with inherited thrombophilia". Blood. 127 (13): 1650–55. doi:10.1182/blood-2015-12-626739. PMID 26837697.
- Egeberg O (June 1965). "Inherited antithrombin deficiency causing thrombophilia". Thromb. Diath. Haemorrh. 13 (2): 516–30. doi:10.1055/s-0038-1656297. PMID 14347873.
- Griffin JH, Evatt B, Zimmerman TS, Kleiss AJ, Wideman C (November 1981). "Deficiency of protein C in congenital thrombotic disease". J. Clin. Invest. 68 (5): 1370–3. doi:10.1172/JCI110385. PMC 370934. PMID 6895379.
- Comp PC, Esmon CT (December 1984). "Recurrent venous thromboembolism in patients with a partial deficiency of protein S". N. Engl. J. Med. 311 (24): 1525–8. doi:10.1056/NEJM198412133112401. PMID 6239102.
- Hughes GR (October 1983). "Thrombosis, abortion, cerebral disease, and the lupus anticoagulant". Br. Med. J. (Clin. Res. Ed.). 287 (6399): 1088–89. doi:10.1136/bmj.287.6399.1088. PMC 1549319. PMID 6414579.
- Sanna G, D'Cruz D, Cuadrado MJ (August 2006). "Cerebral manifestations in the antiphospholipid (Hughes) syndrome". Rheum. Dis. Clin. North Am. 32 (3): 465–90. doi:10.1016/j.rdc.2006.05.010. PMID 16880079.
- Bertina RM, Koeleman BP, Koster T, et al. (May 1994). "Mutation in blood coagulation factor V associated with resistance to activated protein C". Nature. 369 (6475): 64–7. Bibcode:1994Natur.369...64B. doi:10.1038/369064a0. PMID 8164741. S2CID 4314040.
- Poort SR, Rosendaal FR, Reitsma PH, Bertina RM (November 1996). "A common genetic variation in the 3'-untranslated region of the prothrombin gene is associated with elevated plasma prothrombin levels and an increase in venous thrombosis" (PDF). Blood. 88 (10): 3698–703. doi:10.1182/blood.V88.10.3698.bloodjournal88103698. PMID 8916933.