Endoclip
An endoclip is a metallic mechanical device used in endoscopy in order to close two mucosal surfaces without the need for surgery and suturing. Its function is similar to a suture in gross surgical applications, as it is used to join together two disjointed surfaces, but, can be applied through the channel of an endoscope under direct visualization. Endoclips have found use in treating gastrointestinal bleeding (both in the upper and lower GI tract), in preventing bleeding after therapeutic procedures such as polypectomy, and in closing gastrointestinal perforations. Many forms of endoclips exist of different shapes and sizes, including two and three prong devices, which can be administered using single use and reloadable systems, and may or may not open and close to facilitate placement.

Structure and function


The endoclip was first described by Hayashi and Kudoh in 1975,[1] and was termed the "staunch clip". Initial attempts to incorporate the clip into applications in endoscopy (such as clipping bleeding blood vessels) were limited by the applicator system of the clip.[1] However, by 1988, an easy to use applicator delivery system was developed, and a functional reloadable endoclip system was described.[2] This consisted of a stainless steel clip (of size approximately 6 mm long and 1.2 mm wide at the prongs) with a metal deployment device (that could be used to insert the clip into the endoscopic camera, and deployed outside the camera) enclosed in a plastic sheath.[1] These clips were initially reloadable.
Endoclips in use today have a variety of additional shapes and sizes than the original. Clips with two and three prongs (TriClip, Cook Medical[3]) have been described and used for various applications.[4] Rotatable clips have been devised to improve localization of deployment.[5] Also, clips that open and close (as opposed to single-deployment) have also been developed (Resolution Clip, Boston Scientific[6]), and also facilitate the appropriate location of deployment.[7]
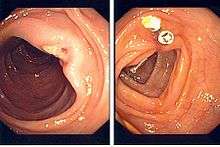
When a treatable lesion is identified on endoscopy (such as a bleeding vessel), an endoclip can be inserted through the channel of the endoscope until the sheathed clip is visible on the endoscopic image, and the handle for deployment handed to the nurse assistant. The clip is unsheathed by retraction at the handle, positioned, and "fired" by the assistant to treat the lesion.
Applications of endoclips
Gastrointestinal bleeding
Endoclips have found a primary application in hemostasis (or the stopping of bleeding) during endoscopy of the upper (through gastroscopy) or lower (through colonoscopy) gastrointestinal tract.[1] Many bleeding lesions have been successfully clipped, including bleeding peptic ulcers,[4] Mallory-Weiss tears of the esophagus,[8] Dieulafoy's lesions,[9] stomach tumours,[10] and bleeding after removal of polyps.[11] Bleeding peptic ulcers require endoscopic treatment if they show evidence of high risk stigmata of re-bleeding, such as evidence of active bleeding or oozing on endoscopy or the presence of a visible blood vessel around the ulcer.[12][13] The alternatives to endoscopic clipping of peptic ulcers are thermal therapy (such as electrocautery to burn the vessel causing the bleeding), or injection of epinephrine to constrict the blood vessel. Comparative studies between endoclips and thermal therapy make the point that endoclips cause less trauma to the mucosa around the ulcer than electrocautery,[14] but no definitive advantage to either approach has reached consensus by gastroenterologists.[15][16]
Other applications
Endoclips have also found an application in preventing bleeding when performing complicated endoscopic procedures. For example, prophylactic clipping of the base of a polyp has been found to be useful in preventing post-polypectomy bleeding, especially in high-risk patients or patients on anticoagulant medications.[17] In addition, clips can be used to close gastrointestinal perforations that may have been caused by complicated therapeutic endoscopy procedures, such as polypectomy, or by the endoscopic procedure itself.[18] Clips have also been used to secure the placement of endoscopic feeding tubes,[19] and to orient the bile duct to assist with endoscopic retrograde cholangiopancreatography, a procedure used to image to bile duct.[20]
Safety
Endoclips have been seen to dislodge between 1 and 3 weeks from deployment,[21] although lengthy clip retention intervals of as high as 26 months have been reported.[1][9] Endoclips are believed to be safe and no major complications (such as perforation or impaction) have been reported with them, although concern has been raised about blocking the outflow of the bile duct if clips are deployed in the duodenum.[1]
References
- Devereaux CE, Binmoeller KF (1999). "Endoclip: closing the surgical gap". Gastrointest. Endosc. 50 (3): 440–2. doi:10.1053/ge.1999.v50.99616. PMID 10462677.
- Binmoeller KF, Thonke F, Soehendra N (1993). "Endoscopic hemoclip treatment for gastrointestinal bleeding". Endoscopy. 25 (2): 167–70. doi:10.1055/s-2007-1010277. PMID 8491134.
- "TriClip Endoscopic Clipping Device". Retrieved 2007-05-15.
- Lin HJ, Lo WC, Cheng YC, Perng CL (2007). "Endoscopic hemoclip versus triclip placement in patients with high-risk peptic ulcer bleeding". Am. J. Gastroenterol. 102 (3): 539–43. PMID 17100962.
- Yoshikane H, Hidano H, Sakakibara A, Niwa Y, Goto H (2000). "Feasibility study on endoscopic suture with the combination of a distal attachment and a rotatable clip for complications of endoscopic resection in the large intestine". Endoscopy. 32 (6): 477–80. doi:10.1055/s-2000-648. PMID 10863916.
- "Resolution Clip". Archived from the original on 2006-11-13. Retrieved 2007-05-15.
- Jensen DM, Machicado GA, Hirabayashi K (2006). "Randomized controlled study of 3 different types of hemoclips for hemostasis of bleeding canine acute gastric ulcers". Gastrointest. Endosc. 64 (5): 768–73. doi:10.1016/j.gie.2006.06.031. PMID 17055872.
- Yamaguchi Y, Yamato T, Katsumi N, Morozumi K, Abe T, Ishida H, Takahashi S (2001). "Endoscopic hemoclipping for upper GI bleeding due to Mallory-Weiss syndrome". Gastrointest. Endosc. 53 (4): 427–30. doi:10.1067/mge.2001.111774. PMID 11275881.
- Teo EK, Fock KM (1998). "Dieulafoy's disease treated by endoscopic haemostatic clipping". J. Gastroenterol. Hepatol. 13 (3): 320–1. doi:10.1111/j.1440-1746.1998.01547.x. PMID 9570248.
- Cheng AW, Chiu PW, Chan PC, Lam SH (2004). "Endoscopic hemostasis for bleeding gastric stromal tumors by application of hemoclip". Journal of Laparoendoscopic & Advanced Surgical Techniques. Part A. 14 (3): 169–71. doi:10.1089/1092642041255522. PMID 15245670.
- Letard JC, Kaffy F, Rousseau D, Nivet JM (2001). "[Post-polypectomy colonic arterial hemorrhage can be treated by hemoclipping]". Gastroenterol. Clin. Biol. (in French). 25 (3): 323–4. PMID 11395682.
- Sung JJ, Chan FK, Lau JY, Yung MY, Leung WK, Wu JC, Ng EK, Chung SC (2003). "The effect of endoscopic therapy in patients receiving omeprazole for bleeding ulcers with nonbleeding visible vessels or adherent clots: a randomized comparison". Ann. Intern. Med. 139 (4): 237–43. doi:10.7326/0003-4819-139-4-200308190-00005. PMID 12965978.
- Lau JY, Sung JJ, Lee KK, Yung MY, Wong SK, Wu JC, Chan FK, Ng EK, You JH, Lee CW, Chan AC, Chung SC (2000). "Effect of intravenous omeprazole on recurrent bleeding after endoscopic treatment of bleeding peptic ulcers". N. Engl. J. Med. 343 (5): 310–6. doi:10.1056/NEJM200008033430501. PMID 10922420.
- Cipolletta L, Bianco MA, Marmo R, Rotondano G, Piscopo R, Vingiani AM, Meucci C (2001). "Endoclips versus heater probe in preventing early recurrent bleeding from peptic ulcer: a prospective and randomized trial". Gastrointest. Endosc. 53 (2): 147–51. doi:10.1067/mge.2001.111386. PMID 11174282.
- Lin HJ, Hsieh YH, Tseng GY, Perng CL, Chang FY, Lee SD (2002). "A prospective, randomized trial of endoscopic hemoclip versus heater probe thermocoagulation for peptic ulcer bleeding". Am. J. Gastroenterol. 97 (9): 2250–4. PMID 12358241.
- Kovacs TO, Jensen DM (2007). "Endoscopic treatment of ulcer bleeding". Current Treatment Options in Gastroenterology. 10 (2): 143–8. doi:10.1007/s11938-007-0066-3. PMID 17391629.
- Friedland S, Soetikno R (2006). "Colonoscopy with polypectomy in anticoagulated patients". Gastrointest. Endosc. 64 (1): 98–100. doi:10.1016/j.gie.2006.02.030. PMID 16813811.
- Shimizu Y, Kato M, Yamamoto J, Nakagawa S, Komatsu Y, Tsukagoshi H, Fujita M, Hosokawa M, Asaka M (2004). "Endoscopic clip application for closure of esophageal perforations caused by EMR". Gastrointest. Endosc. 60 (4): 636–9. doi:10.1016/S0016-5107(04)01960-1. PMID 15472698.
- Frizzell E, Darwin P (2006). "Endoscopic placement of jejunal feeding tubes by using the Resolution clip: report of 2 cases". Gastrointest. Endosc. 64 (3): 454–6. doi:10.1016/j.gie.2006.02.051. PMID 16923504.
- Scotiniotis I, Ginsberg GG (1999). "Endoscopic clip-assisted biliary cannulation: externalization and fixation of the major papilla from within a duodenal diverticulum using the endoscopic clip fixing device". Gastrointest. Endosc. 50 (3): 431–6. doi:10.1053/ge.1999.v50.97369. PMID 10462673.
- Binmoeller KF, Grimm H, Soehendra N (1993). "Endoscopic closure of a perforation using metallic clips after snare excision of a gastric leiomyoma". Gastrointest. Endosc. 39 (2): 172–4. doi:10.1016/S0016-5107(93)70060-7. PMID 8495838.