Gray matter heterotopia
Gray matter heterotopias are neurological disorders caused by clumps of gray matter (nodules of neurons) located in the wrong part of the brain.[1] A grey matter heterotopia is characterized as a type of focal cortical dysplasia. The neurons in heterotopia appear to be normal, except for their mislocation; nuclear studies have shown glucose metabolism equal to that of normally positioned gray matter.[2] The condition causes a variety of symptoms, but usually includes some degree of epilepsy or recurring seizures, and often affects the brain's ability to function on higher levels. Symptoms range from nonexistent to profound; the condition is occasionally discovered as an incidentaloma when brain imaging performed for an unrelated problem and has no apparent ill effect on the patient. At the other extreme, heterotopia can result in severe seizure disorder, loss of motor skills, and mental retardation. Fatalities are practically unknown, other than the death of unborn male fetuses with a specific genetic defect.
Preliminary Material: Neurological Development of the Human Fetus
The development of the brain in the human fetus is extraordinarily complex and is still not fully understood. Neural matter originates in the outer, ectodermic layer of the gastrula; thus, it originates from the cell layer primarily responsible for skin, hair, nails, etc., rather than from the layers that develop into other internal organs. The nervous system originates as a tiny, simple open tube called the neural tube;[3] the front of this tube develops into the brain (and retinas of the eye), while the spinal cord develops from the very back end.
Neurons begin to form early, but most of them become structural rather than active nerve cells. The brain generally forms from the inside-out, especially in the case of the neocortex. The difficulties arising from this are readily apparent, as each successive layer of cells must travel through the previous layer to reach its destination. Therefore, nervous tissue develops ladders made of radial glial cells that neurons climb, through the previous layers, to reach their proper destination. Some destinations, such as the cerebral cortex, even have "placeholder" neurons that travel up the ladder to form a structure; when the final neurons germinate, they find a correct placeholder and then the placeholder cell dies.
Heterotopia
The complexity of neural development makes it fraught with opportunities for error. Grey matter heterotopia[4] is such an example. It is believed that gray matter heterotopia are caused by arrested migration of neurons to the cerebral cortex; that is, when neurons that are supposed to form part of the cerebral cortex.[5] fail to climb to the end of their ladder correctly and are permanently situated in the wrong location.
Gray matter heterotopia are common malformations of cortical development classed as neuronal migration disorders. Heterotopias are classed in two groups: nodular and diffuse. Nodular types are subependymal and subcortical; diffuse types are termed band heterotopias. Affected patients are generally divided into three groups, depending on the location of the formation: subependymal, subcortical, and band heterotopia. In addition, especially with heterotopia that are genetically linked, there are gender differences, men suffering more severe symptoms than women with similar formations.
In general, band heterotopia, also known as double cortex syndrome,[6] are seen exclusively in women; men with a mutation of the related gene (called XLIS or DCX) usually die in utero or have a much more severe brain anomaly. Symptoms in affected women vary from normal to severe developmental delay or mental retardation; the severity of the syndrome is related to the thickness of the band of arrested neurons. Nearly all affected patients that come to medical attention have epilepsy, with partial complex and atypical absence epilepsy being the most common syndromes. Some of the more severely affected patients develop drop attacks.
Periventricular or subependymal
Periventricular means beside the ventricle, while subependymal (also spelled subepydymal) means beneath the ependyma; because the ependyma is the thin epithelial sheet lining the ventricles of the brain, these two terms are used to define heterotopia occurring directly next to a ventricle. This is by far the most common location for heterotopia. Patients with isolated subependymal heterotopia usually present with a seizure disorder in the second decade of life.
Subependymal heterotopia present in a wide array of variations. They can be a small single node or a large number of nodes, can exist on either or both sides of the brain at any point along the higher ventricle margins, can be small or large, single or multiple, and can form a small node or a large wavy or curved mass.
Symptomatic women with subependymal heterotopia typically present with partial epilepsy during the second decade of life; development and neurologic examinations up to that point are typically normal. Symptoms in men with subependymal heterotopia vary, depending on whether their disease is linked to their X-chromosome. Men with the X-linked form more commonly have associated anomalies, which can be neurological or more widespread, and they usually suffer from developmental problems. Otherwise (i.e., in non-X-linked cases) the symptomology is similar in both sexes.
Focal subcortical
Subcortical heterotopia form as distinct nodes in the white matter, "focal" indicating specific area. In general, patients present fixed neurologic deficits and develop partial epilepsy between the ages of 6 and 10. The more extensive the subcortical heterotopia, the greater the deficit; bilateral heterotopia are almost invariably associated with severe developmental delay or mental retardation. The cortex itself often suffers from an absence of gray matter and may be unusually thin or lack deep sulci. Subependymal heterotopia are frequently accompanied by other structural abnormalities, including an overall decrease in cortical mass. Patients with focal subcortical heterotopia have a variable motor and intellectual disturbance depending on the size and site of the heterotopion.
Band form
Like focal subcortical heterotopia, "band" heterotopia form in the white matter beneath the cortex, but the gray matter is more diffuse and is symmetric between the hemispheres. On imaging, band heterotopia appears as bands of gray matter situated between the lateral ventricle and cerebral cortex and separated from both by a layer of normal appearing white matter. Band heterotopia may be complete, surrounded by simple white matter, or partial. The frontal lobes seem to be more frequently involved when it is partial. Patients with band heterotopia may present at any age with variable developmental delay and seizure disorder, which vary widely in severity.
Subcortical band heterotopia, also known as “double cortex” syndrome, refers to a band of subcortical heterotopia neurons, located midway between the ventricles and the cerebral cortex. The disorder is seen primarily in females and typically causes varying degrees of mental retardation and almost all of them have epilepsy. Approximately two thirds of patients with epilepsy ultimately develop intractable seizures. MRI of the brain in subcortical band heterotopia demonstrates two parallel layers of gray matter: a thin outer ribbon and a thick inner band, separated by a very thin layer of white matter between them. The severity of epilepsy and developmental delay is directly correlated with the degree of migration arrest, as indicated by the thickness of the subcortical band heterotopia.
Subcortical band heterotopia is caused by mutations in the microtubule-associated DCX gene. The DCX protein is thought to direct neuronal migration by regulating the organization and stability of microtubules, necessary for neuronal motility. The malformation is seen only in females, as the gene is found on the X-chromosome. Since there are two X chromosomes in females, after X-inactivation, only some neurons lose doublecortin function. These neurons with the mutant DCX gene fail to migrate into the cortex and thus form the underlying heterotopic band, while neurons which express the normal gene successfully migrate out to the cortical plate. Males with DCX mutations develop classical lissencephaly.
Diagnosis
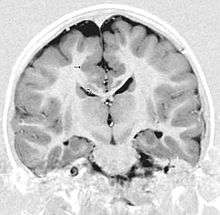
Detection of heterotopia generally occurs when a patient receives brain imaging—usually an MRI or CT scan—to diagnose seizures that are resistant to medication. Correct diagnosis requires a high degree of radiological skill, due to the heterotopia's resemblance to other masses in the brain.
Treatment
When seizures are present in any forms of cortical dysplasia, they are resistant to medication. Frontal lobe resection provides significant relief from seizures to a minority of patients with periventricular lesions.
Prognosis
In general, gray matter heterotopia is fixed in both its occurrence and symptoms; that is, once symptoms occur, it does not tend to progress. Varying results from surgical resection of the affected area have been reported. Although such surgery cannot reverse developmental disabilities, it may provide full or partial relief from seizures.
Heterotopia are most commonly isolated anomalies, but may be part of a number of syndromes, including chromosomal abnormalities and fetal exposure to toxins (including alcohol).
Footnotes
- Gaillard, Frank. "Grey matter heterotopia | Radiology Reference Article | Radiopaedia.org". Radiopaedia.
- uhrad.com - Neuroradiology Imaging Teaching Files
- For a good illustration of the neural tube, see https://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=dbio.figgrp.2886
- "Hetero" is from Greek "different" (e.g., heterosexual = "different sex") and "topia" from "place" (e.g., utopia = "ideal place"); thus, heterotopia means "different place".
- Many parts of the brain, in addition to the cerebrum, contain grey matter.
- Gaillard, Frank. "Band heterotopia | Radiology Reference Article | Radiopaedia.org". Radiopaedia.
Further reading
- GeneReviews/NCBI/NIH/UW entry on X-Linked Periventricular Heterotopia
- Ferland, Russell J.; Batiz, Luis Federico; Neal, Jason; Lian, Gewei; Bundock, Elizabeth; Lu, Jie; Hsiao, Yi-Chun; Diamond, Rachel; Mei, Davide; Banham, Alison H.; Brown, Philip J.; Vanderburg, Charles R.; Joseph, Jeffrey; Hecht, Jonathan L.; Folkerth, Rebecca; Guerrini, Renzo; Walsh, Christopher A.; Rodriguez, Esteban M.; Sheen, Volney L. (2009). "Disruption of neural progenitors along the ventricular and subventricular zones in periventricular heterotopia". Human Molecular Genetics. 18 (3): 497–516. doi:10.1093/hmg/ddn377. PMC 2722192. PMID 18996916.