Appendectomy
An appendectomy, also termed appendicectomy, is a surgical operation in which the vermiform appendix (a portion of the intestine) is removed. Appendectomy is normally performed as an urgent or emergency procedure to treat complicated acute appendicitis.[1]
| Appendectomy | |
|---|---|
 An appendectomy in progress | |
| Other names | Appendisectomy, appendicectomy |
| Specialty | General surgery |
| Uses | Appendicitis |
| Complications | Infection, bleeding |
| Approach | Laparoscopic, open |
Appendectomy may be performed laparoscopically (as minimally invasive surgery) or as an open operation.[2] Over the 2010s, surgical practice has increasingly moved towards routinely offering laparoscopic appendicectomy; for example in the United Kingdom over 95% of adult appendicectomies are planned as laparoscopic procedures.[3] Laparoscopy is often used if the diagnosis is in doubt, or in order to leave a less visible surgical scar. Recovery may be slightly faster after laparoscopic surgery, although the laparoscopic procedure itself is more expensive and resource-intensive than open surgery and generally takes longer. Advanced pelvic sepsis occasionally requires a lower midline laparotomy. In US adults, the 30-day mortality after appendectomy was 1.8%.[4]
Both uncomplicated (non-perforated) and complicated (perforated) appendicitis should undergo prompt surgical intervention.[1] The difference in treatment occurs post-operatively with respect to the length of time the antibiotics are administered. For uncomplicated appendicitis, antibiotics should be continued up to 24 hours post-operatively. For complicated appendicitis, antibiotics should be continued for anywhere between 3 and 7 days.[1] Delay of appendectomy 24 hours after admission for symptoms of appendicitis has not shown to increase risk of perforation or other complications.[5]
Procedure



In general terms, the procedure for an open appendectomy is:
- Antibiotics are given immediately if signs of actual sepsis are seen (in appendicitis, sepsis and bacteremia usually only occurs at some point after rupture, once peritonitis has begun), or if there is reasonable suspicion that the appendix has ruptured (e.g., on imaging) or if the onset of peritonitis- which will lead to full sepsis if not quickly treated- is suspected; otherwise, a single dose of prophylactic intravenous antibiotics is given immediately before surgery.[6]
- General anaesthesia is induced, with endotracheal intubation and full muscle relaxation, and the patient is positioned supine.[6]
- The abdomen is prepared and draped and is examined under anesthesia.[6]
- If a mass is present, the incision is made over the mass. Otherwise, the incision is made over McBurney's point (one-third of the way from the anterior superior iliac spine to the umbilicus), which represents the most common position of the base of the appendix.[6]
- The various layers of the abdominal wall are opened. In order to preserve the integrity of abdominal wall, the external oblique aponeurosis is split along the line of its fibers, as is the internal oblique muscle. As the two run at right angles to each other, this reduces the risk of later incisional hernia.[6]
- On entering the peritoneum, the appendix is identified, mobilized, and then ligated and divided at its base.[6]
- Some surgeons choose to bury the stump of the appendix by inverting it so it points into the caecum.[6]
- Each layer of the abdominal wall is then closed in turn.[6]
- The skin may be closed with staples or stitches.[6]
- The wound is dressed.
- The patient is brought to the recovery room.
Incisions
The standardization of an incision is not best practice when performing an appendectomy given that the appendix is a mobile organ.[6] A physical exam should be performed prior to the operation and the incision should be chosen based on the point of maximal tenderness to palpation.[6]
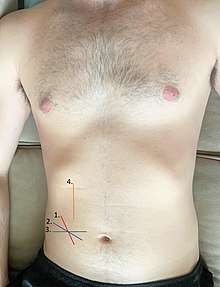
These incisions are placed for appendectomy:
- McBurney's incision, also known as grid iron incision
- Lanz incision
- Rutherford Morison incision
- Paramedian incision

Over the past decade, the outcomes of laparoscopic appendectomies have compared favorably to those for open appendectomies because of decreased pain, fewer postoperative complications, shorter hospitalization, earlier mobilization, earlier return to work, and better cosmesis; however, despite these advantages, efforts are still being made to decrease abdominal incision and visible scars after laparoscopy.[7] Recent research has led to the development of natural orifice transluminal endoscopic surgery (NOTES); however, numerous difficulties need to be overcome before a wider clinical application of NOTES is adopted, including complications such as the opening of hollow viscera, failed sutures, a lack of fully developed instrumentation, and the necessity of reliable cost-benefit analyses.[8][8]
Many surgeons have attempted to reduce incisional morbidity and improve cosmetic outcomes in laparoscopic appendectomy by using fewer and smaller ports. Kollmar et al. described moving laparoscopic incisions to hide them in the natural camouflages like the suprapubic hairline to improve cosmesis. Additionally, reports in the literature indicate that minilaparoscopic appendectomy using 2– or 3-mm or even smaller instruments along with one 12-mm port minimizes pain and improves cosmesis. More recently, studies by Ates et al. and Roberts et al. have described variants of an intracorporeal sling-based single-port laparoscopic appendectomy with good clinical results.[8]
Also, a trend is increasing towards single-incision laparoscopic surgery (SILS), using a special multiport umbilical trocar.[9] With SILS, a more conventional view of the field of surgery is seen compared to NOTES. The equipment used for SILS is familiar to surgeons already doing laparoscopic surgery. Most importantly, it is easy to convert SILS to conventional laparoscopy by adding a few trocars; this conversion to conventional laparoscopy is called 'port rescue'. SILS has been shown to be feasible, reasonably safe, and cosmetically advantageous, compared to standard laparoscopy; however, this newer technique involves specialized instruments and is more difficult to learn because of a loss of triangulation, clashing of instruments, crossing of instruments (cross triangulation), and a lack of maneuverability.[8] The additional problem of decreased exposure and the added financial burden of procuring special articulating or curved coaxial instruments exist. SILS is still evolving, being used successfully in many centres, but with some way to go before it becomes mainstream. This limits its widespread use, especially in rural or peripheral centres with limited resources.[8]
Pregnancy
Appendicitis is the most common emergent general surgery related problem to arise during pregnancy. There is a natural elevation in white blood cell count in addition to anatomical changes of the appendix that occur during pregnancy.[10] These findings, in addition to non-specific abdominal symptoms make appendicitis difficult to diagnose. Appendicitis develops most commonly in the second trimester.[2] If appendicitis develops in a pregnant woman, an appendectomy is usually performed and should not harm the fetus.[11] The risk of premature delivery is about 10%.[12] The risk of fetal death in the perioperative period after an appendectomy for early acute appendicitis is 3 to 5%. The risk of fetal death is 20% in perforated appendicitis.[13]
There has been debate regarding which surgical approach is preferred during pregnancy. Overall, there is no increased risk of fetal loss or preterm delivery with the laparoscopic approach (LA) as compared to the open approach (OA). However, the LA was associated with shorter length of stay in the hospital as well as reduced risk of wound infection.[2]
Patient positioning is of utmost importance to ensure safety of the fetus during the procedure. This is especially important during the third trimester due to the potential of compression of the inferior vena cava leading by the enlarged uterus. Placing the patient in a 30-degree left lateral decubitus position alleviates this pressure and prevents fetal distress.[10]
One area of concern related to the LA during pregnancy is pneumoperitoneum. This causes an increase in the intra-abdominal pressure, leading to decreased venous return and therefore, decreased cardiac output. The decreased cardiac output may lead to fetal acidosis and cause distress. However, an animal pregnancy model demonstrated that a 10-12mmHg insufflation pressure demonstrated no adverse effects on the fetus. SAGES (Society of American Gastrointestinal and Endoscopic Surgeons) currently recommends an insufflation pressure of 10-15mmHg during pregnancy.[2]
Recovery


A study from 2010 found that the average hospital stay for people with appendicitis in the United States was 1.8 days. For people with a perforated (ruptured) appendix, the average length of stay was 5.2 days.[14]
Recovery time from the operation varies from person to person. Some take up to three weeks before being completely active; for others, it can be a matter of days. In the case of a laparoscopic operation, the patient has three stapled scars of about an inch (2.5 cm) in length, between the navel and pubic hair line. When an open appendectomy has been performed, the patient has a 2– to 3-inch (5–7.5 cm) scar, which will initially be heavily bruised.[15]
Complications
One of the most common post-operative complications associated with an appendectomy is the development of a surgical site infection (SSI).[16] Signs and symptoms indicative of a superficial SSI are redness, swelling, and tenderness surrounding the incision and are most likely to arise on post-operative day 4 or 5. These symptoms oftentimes precede fluid drainage from the incision. Tenderness extending beyond the redness that surrounds the incision, in addition to the development of cutaneous vesicles or bullae may be indicative of a deep SSI.[16]
Patients with complicated appendicitis (perforated appendicitis) are more likely to develop a SSI, abdominal abscess, or pelvic abscess during the post-operative period. Placement of an abdominal drain was originally thought to reduce the risk of these post-operative complications. However, abdominal drains have not been found to play a significant role in reducing SSIs and have lead to increased length of stay in the hospital in addition to increased cost of the operation.[17]
Frequency
About 327,000 appendectomies were performed during U.S. hospital stays in 2011, a rate of 10.5 procedures per 10,000 population. Appendectomies accounted for 2.1% of all operating-room procedures in 2011.[18]
History
.JPG)
The first recorded successful appendectomy was on December 6, 1735, at St. George's Hospital in London, when French surgeon Claudius Amyand described the presence of a perforated appendix within the inguinal hernial sac of an 11-year-old boy.[5] The organ had apparently been perforated by a pin the boy had swallowed. The patient, Hanvil Andersen, made a recovery and was discharged a month later.[19]
Harry Hancock performed the first abdominal surgery for appendicitis in 1848, but he did not remove the appendix.[20] In 1889 in New York City, Charles McBurney described the presentation and pathogenesis of appendicitis accurately and developed the teaching that an early appendectomy was the best treatment to avoid perforation and peritonitis.
Some cases of autoappendectomies have occurred. One was attempted by Evan O'Neill Kane in 1921, but the operation was completed by his assistants. Another was Leonid Rogozov, who had to perform the operation on himself as he was the only doctor on a remote Antarctic base.[21][22]
On September 13, 1980, Kurt Semm performed the first laparoscopic appendectomy opening up the path for a much wider application of minimally invasive surgery.[23][24]
Cost
United States
While appendectomy is a standard surgical procedure, its cost has been found to vary considerably in the United States. A 2012 study analyzed 2009 data from nearly 20,000 adult patients treated for appendicitis in California hospitals. Researchers examined “only uncomplicated episodes of acute appendicitis” that involved “visits for patients 18 to 59 years old with hospitalization that lasted fewer than four days with routine discharges to home.” The lowest charge for removal of an appendix was $1,529 and the highest $182,955, more than 120 times greater. The median charge was $33,611.[25][26] While the study was limited to California, the researchers indicated that the results were applicable anywhere in the United States. Many, but not all, patients are covered by some sort of medical insurance.[27]
A study by the Agency for Healthcare Research and Quality found that in 2010, the average cost for a stay in the United States involving appendicitis was $7,800. For stays where the appendix had ruptured, the average cost was $12,800. The majority of patients seen in the hospital were covered by private insurance.[14]
See also
- List of surgeries by type
References
- Backbourne, Lorne. Surgical Recall. Wolters Kluwer. pp. 198–203.
- Lee, Seung Hwan; Lee, Jin Young; Choi, Yoon Young; Lee, Jae Gil (2019-04-25). "Laparoscopic appendectomy versus open appendectomy for suspected appendicitis during pregnancy: a systematic review and updated meta-analysis". BMC Surgery. 19 (1): 41. doi:10.1186/s12893-019-0505-9. ISSN 1471-2482. PMC 6482586. PMID 31023289.
- RIFT Study Group on behalf of the West Midlands Research Collaborative (3 December 2019). "Evaluation of appendicitis risk prediction models in adults with suspected appendicitis". BJS (British Journal of Surgery). n/a (n/a): 73–86. doi:10.1002/bjs.11440. ISSN 1365-2168. PMC 6972511. PMID 31797357.
- Margenthaler JA, Longo WE, Virgo KS, et al. (Jul 2003). "Risk Factors for Adverse Outcomes After the Surgical Treatment of Appendicitis in Adults". Ann. Surg. 238 (1): 59–66. doi:10.1097/01.SLA.0000074961.50020.f8. PMC 1422654. PMID 12832966.
- Yelon, Jay A.; Luchette, Fred A. (2013). Geriatric Trauma and Critical Care. Springer Science & Business Media. ISBN 9781461485018.
- Zollinger, Robert (2016). Zollinger's Atlas of Surgical Operations. McGraw-Hill Education. p. 162. ISBN 978-0-07-179756-6.
- Zollinger, Robert (2016). Zollinger's Atlas of Surgical Operations. McGraw-Hill Education. p. 49. ISBN 978-0-07-179756-6.
- Ashwin, Rammohan; Paramaguru, Jothishankar; Manimaran, A. B.; Naidu, R. M. (2012). "Two-port vs. three-port laparoscopic appendicectomy: A bridge to least invasive surgery". Journal of Minimal Access Surgery.
- Far, Sasan Saeed; Miraj, Sepide (October 2016). "Single-incision laparoscopy surgery: a systematic review". Electronic Physician. 8 (10): 3088–3095. doi:10.19082/3088. ISSN 2008-5842. PMC 5133033. PMID 27957308.
- "Sign In | Health Library". lwwhealthlibrary.com. Retrieved 2020-01-11.
- Factors That Develop During Pregnancy at Merck Manual of Diagnosis and Therapy Home Edition
- Schwartz Book of General Surgery
- Sabiston Textbook of Surgery 2007.
- Barrett M. L., Hines A. L., Andrews R. M. Trends in Rates of Perforated Appendix, 2001–2010. HCUP Statistical Brief #159. Agency for Healthcare Research and Quality, Rockville, MD. July 2013.
- Surgery 2
- Townsend, Courtney (2017). Sabiston Textbook of Surgery. Elsevier, Inc. pp. 241–280.
- Cheng, Yao; Zhou, Shiyi; Zhou, Rongxing; Lu, Jiong; Wu, Sijia; Xiong, Xianze; Ye, Hui; Lin, Yixin; Wu, Taixiang; Cheng, Nansheng (2015-02-07). "Abdominal drainage to prevent intra-peritoneal abscess after open appendectomy for complicated appendicitis". The Cochrane Database of Systematic Reviews (2): CD010168. doi:10.1002/14651858.CD010168.pub2. ISSN 1469-493X. PMID 25914903.
- Weiss A. J.; Elixhauser A.; Andrews R. M. (February 2014). "Characteristics of Operating Room Procedures in U.S. Hospitals, 2011". HCUP Statistical Brief #170. Rockville, MD: Agency for Healthcare Research and Quality.
- Amyand, Claudius (1735). "Of an inguinal rupture, with a pin in the appendix caeci, incrusted with stone; and some observations on wounds in the guts". Philosophical Transactions of the Royal Society of London. 39 (443): 329–336. doi:10.1098/rstl.1735.0071. Archived from the original on 2017-05-15. Retrieved 2016-10-12.
- Schwartz's principles of surgery (9 ed.). New York: McGraw-Hill, Medical Pub. Division. 2010. p. 1075. ISBN 9780071547697.
- Rogozov V.; Bermel N. (2009). "Auto-appendectomy in the Antarctic: case report". BMJ. 339: b4965. doi:10.1136/bmj.b4965. PMID 20008968.
- Lentati, Sara (May 5, 2015). "The man who cut out his own appendix". BBC News.
- Grzegorz S. Litynski (1998). "Kurt Semm and the Fight against Skepticism: Endoscopic Hemostasis, Laparoscopic Appendectomy, and Semm's Impact on the "Laparoscopic Revolution"". JSLS. 2 (3): 309–13. PMC 3015306. PMID 9876762.
- Semm K (March 1983). "Endoscopic Appendectomy". Endoscopy. 15 (2): 59–64. doi:10.1055/s-2007-1021466. PMID 6221925.
- "Health Care as a 'Market Good'? Appendicitis as a Case Study". JournalistsResource.org, retrieved April 25, 2012
- Hsia, Renee Y.; Kothari, Abbas H.; Srebotnjak, Tanja; Maselli, Judy (2012). "Health Care as a 'Market Good'? Appendicitis as a Case Study". Archives of Internal Medicine. 172 (10): 818–9. doi:10.1001/archinternmed.2012.1173. PMC 3624019. PMID 22529183.
- Tanner, Lindsey (April 24, 2012). "Study finds appendectomy could cost as much as house". Florida Today. Melbourne, Florida. pp. 6A.
External links
| Wikimedia Commons has media related to Appendectomy. |
- Open Appendectomy: Operative procedure video
- Laparoscopic Appendectomy Video (includes case presentation)
- Open appendectomy, appendectomy – part of the operative how-to series, explaining the steps in carrying out an open appendectomy
- Open & Laparoscopic appendectomy, appendectomy
- A video of the procedure
- Another video of the procedure (either requires Windows Media Player and will not load in Firefox 1.5; or use with any player that can play .wmv files)
| Classification | |
|---|---|
| External resources |