Prostatic artery embolization
Prostatic artery embolization (PAE, or prostate artery embolisation) is a developing non-surgical technique for treatment of benign prostatic hypertrophy (BPH).[1] Although there is increasing research on PAE, use of the technique remains at an incipient stage.
The procedure involves blocking the blood flow of small branches of the prostatic arteries using microparticles injected via a small catheter,[2] to decrease the size of the prostate gland. It is a minimally invasive therapy which can be performed with local anesthesia, as an outpatient procedure.[2]
Treatment of lower urinary tract symptoms
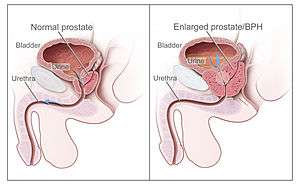
Men with an enlarged prostate may suffer from symptoms of lower urinary tract obstruction, such as sensation of incomplete urination, inability to urinate, weak urinary stream, or having to urinate frequently (often awakening from sleep).[3] If the symptoms cause a significant disruption to quality of life, a man may undergo initial treatment by oral medication, such as alpha-1 receptor blockers, 5-alpha-reductase inhibitors, or phosphodiesterase-5 enzyme inhibitors. Those with severe/progressive symptoms or those who do not experience symptom relief from medication have traditionally been considered for surgical intervention, with transurethral resection of the prostate or TURP as the standard of care.
However, there are problems with both medical and surgical treatments, including undesired side effects and variable effectiveness. For example, sexual dysfunction and orthostatic hypotension are side effects of 5-alpha-reductase inhibitors.[4] Prostatic artery embolization is an emerging treatment alternative which avoids the risks of systemic medication and of surgery.
The first report of selective prostatic artery embolization resulting in relief of prostate gland obstruction was published in 2000.[5] Since then, prospective trials with small numbers of patients, up to approximately 200 patients/trial, have been carried out internationally. Results show that PAE decreases prostate gland size, prostate specific antigen level, peak urinary flow, post-void residual, and subject urinary symptoms.[6]
Adverse Effects
As PAE is a relatively new procedure, more data is needed to determine the incidence of adverse effects. The majority of adverse effects during PAE are likely due to non-target embolization, and are generally self-limited in nature.
A post-embolization syndrome, consisting of pain, mild fever, malaise, nausea, vomiting and night sweats, is commonly observed after the procedure, and is treated with NSAIDS and other forms of analgesia.
According to a systematic review of trials, the most common adverse effects include acute urinary retention, rectal bleeding, pain, blood in the urine/sperm, and urinary tract infection. Serious complications are uncommon, and include arterial dissection, bladder wall ischemia, and persistent urinary tract infection.
One single-center prospective study reported an overall complication rate up to 20.6%, with mostly minor complications including hematospermia, diarrhea, and urethral trauma from foley insertion, with one major complication of UTI requiring intravenous antibiotics.[7]
Procedure
After local anesthesia is placed, an interventional radiologist obtains access to the arterial system by piercing the femoral or radial artery, usually under ultrasound guidance, with a hollow needle known as a trocar. Through the needle a guidewire is threaded and subsequently the trocar is removed. A cannula is slid over the guidewire and once in place the guidewire is removed. This cannula allows a sheath to be inserted into the artery.8 Contrast material is injected through the sheath under fluoroscopic imaging which outlines the anatomy of the blood vessels. This technique is used to help locate the prostatic artery and advance the catheter to the ostium of the prostatic artery. Polyvinyl alcohol particles are then injected into the prostatic artery. They function by causing embolization (blockage of the artery) preventing blood flow to the prostate, functionally resulting in reduced prostate size.[8]
See also
- Photoselective vaporization of the prostate
- Transurethral needle ablation
- Transurethral resection of the prostate
References
- "Prostate artery embolisation for benign prostatic hyperplasia | Guidance and guidelines | NICE". www.nice.org.uk. Retrieved 2017-03-08.
- "Prostate artery embolisation for benign prostatic hyperplasia | 2-The-procedure | Guidance and guidelines | NICE". www.nice.org.uk. Retrieved 2017-03-08.
- Norman, RW; Nickel, JC; et al. (1994). ""Prostate-related symptoms" in Canadian men 50 years of age or older: prevalence and relationships among symptoms". Br J Urol. 74 (5): 542–550. doi:10.1111/j.1464-410x.1994.tb09181.x.
- Traish, AM; Hassani, J; Guay, AT; et al. (2011). "Adverse Side Effects of 5α‐Reductase Inhibitors Therapy: Persistent Diminished Libido and Erectile Dysfunction and Depression in a Subset of Patients". J Sex Med. 8 (3): 872–884. doi:10.1111/j.1743-6109.2010.02157.x. PMID 21176115.
- DeMeritt, John S.; Elmasri, Fakhir F.; Esposito, Michael P.; Rosenberg, Gene S. (June 2000). "Relief of Benign Prostatic Hyperplasia-related Bladder Outlet Obstruction after Transarterial Polyvinyl Alcohol Prostate Embolization". Journal of Vascular and Interventional Radiology. 11 (6): 767–770. doi:10.1016/S1051-0443(07)61638-8.
- Kuang, Michelle; Vu, Anthony; Athreya, Sriharsha (28 December 2016). "A Systematic Review of Prostatic Artery Embolization in the Treatment of Symptomatic Benign Prostatic Hyperplasia". CardioVascular and Interventional Radiology. 40 (5): 655–663. doi:10.1007/s00270-016-1539-3. PMID 28032133.
- Assis, AM; Rodrigues, VCP; Yoshinaga, EM; et al. (2015). "Prostatic artery embolization (PAE) for treatment of benign prostatic hyperplasia in patients with prostates exceeding 90 g: a prospective single center study". J Vasc Interv Radiol. 26 (1): 87–93. doi:10.1016/j.jvir.2014.10.012.
- Wang, MQ; Guo, LP; Zhang, GD; et al. (2015). "Prostatic arterial embolization for the treatment of lower urinary tract symptoms due to large (>80 mL) benign prostatic hyperplasia: results of midterm follow-up from Chinese population". BMC Urol. 2015 (15): 33. doi:10.1186/s12894-015-0026-5. PMC 4403829. PMID 25887036.