Pentalogy of Cantrell
Pentalogy of Cantrell (or thoraco-abdominal syndrome) is a rare[1] syndrome that causes defects involving the diaphragm, abdominal wall, pericardium, heart and lower sternum.
| Pentalogy of Cantrell | |
|---|---|
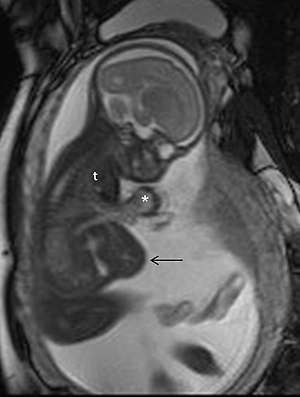 | |
| MRI in pregnancy in a case of pentalogy of Cantrell, showing ectopia cordis (*), partial herniation of the liver (arrow), and a small thoracic cavity (t) | |
| Specialty | Medical genetics |
Presentation

There are five characteristic findings in pentalogy of Cantrell:
- an abdominal wall defect,
- lower sternal defect,
- congenital heart malformations,
- absence of the diaphragmatic pericardium,
- and an anterior diaphragmatic defect.[2]
Abdominal wall defects in pentalogy of Cantrell occur above the umbilicus (supraumbilical) and in the midline, and have a wide range of presentations. Diastasis recti, hernias, and omphalocele have all been described in conjunction with the pentalogy.[2]
Sternal defects too have a range of presentations, from absence of the xiphoid process to shortened or cleft sternum. If the sternal defect is large enough, the neonate may have ectopia cordis, in which the heart is located outside of the thorax.[2]
Many congenital heart malformations have been described in conjunction with pentalogy of Cantrell. The most common is ventricular septal defect, found in 72% of cases. Others include atrial septal defect, cardiac diverticulum, pulmonic stenosis, double outlet right ventricle, tetralogy of Fallot, dextrocardia, and transposition of the great vessels.[2]
Causes
Most cases of pentalogy of Cantrell are idiopathic (no known cause). However, some cases have been described with a genetic linkage to a locus at Xq25-q26.1.[3]
Diagnosis
A diagnosis of pentalogy of Cantrell can often be made before birth (prenatally) sometimes using a fetal ultrasound to detect some of the defects associated with pentalogy of Cantrell. Echocardiography is usually performed to evaluate the extent of the involvement of the heart.
Magnetic resonance imaging (MRI) may also be performed to assess the degree of certain anomalies such as abdominal wall and pericardial defects. An MRI uses a magnetic field and radio waves to produce cross-sectional images of particular organs and bodily tissues.
Treatment
The treatment of pentalogy of Cantrell is directed toward the specific symptoms that are apparent in each individual. Surgical intervention for cardiac, diaphragmatic and other associated defects is necessary. Affected infants will require complex medical care and may require surgical intervention. In most cases, pentalogy of Cantrell is fatal without surgical intervention. However, in some cases, the defects are so severe that the individual dies regardless of the medical or surgical interventions received.
The specific treatment strategy will vary from one infant to another based upon various factors, including the size and type of abdominal wall defect, the specific cardiac anomalies that are present, and the particular type of ectopia cordis. Surgical procedures that may be required shortly after birth include repair of an omphalocele. At this time, physicians may also attempt to repair certain other defects including defects of the sternum, diaphragm and the pericardium.
In severe cases, some physicians advocate for a staged repair of the defects associated with pentalogy of Cantrell. The initial operation immediately after birth provides separation of the peritoneal and pericardial cavities, coverage of the midline defect and repair of the omphalocele. After appropriate growth of the thoracic cavity and lungs, the second stage consists of the repair of cardiac defects and return of the heart to the chest. Eventually, usually by age 2 or 3, reconstruction of the lower sternum or epigastrium may be necessary.
Other treatment of pentalogy of Cantrell is symptomatic and supportive.
Epidemiology
Pentalogy of Cantrell occurs in 1/65,000 to 1/200,000 live births.[2]
History
It was first characterized in 1958.[4]
A 2010 study concluded that the 13th-century Christian saint Rose of Viterbo died of complications of Pentalogy of Cantrell.[5]
References
- Katranci AO, Görk AS, Rizalar R, et al. (1998). "Pentalogy of Cantrell". Indian J Pediatr. 65 (1): 149–53. doi:10.1007/BF02849710. PMID 10771959.
- "Orphanet: Pentalogy of Cantrell". www.orpha.net. Retrieved 2017-07-29.
- "OMIM Entry - % 313850 - THORACOABDOMINAL SYNDROME; THAS". www.omim.org. Retrieved 2018-10-31.
- CANTRELL JR, HALLER JA, RAVITCH MM (November 1958). "A syndrome of congenital defects involving the abdominal wall, sternum, diaphragm, pericardium, and heart". Surg Gynecol Obstet. 107 (5): 602–14. PMID 13592660.
- D'Anastasio PhD, Ruggero; et al. (19 June 2010). "The Heart of Santa Rosa". The Lancet. 375 (9732): 2168. doi:10.1016/s0140-6736(09)60729-7. PMID 20541795.
External links
| Classification | |
|---|---|
| External resources |