Clearing the cervical spine
Clearing the cervical spine is the process by which medical professionals determine whether cervical spine injuries exist, mainly regarding cervical fracture. It is generally performed in cases of major trauma. This process can take place in the emergency department or in the field by appropriately trained EMS personnel.
| Clearing the cervical spine | |
|---|---|
| Calculator | MDCalc |
If the patient is obtunded, i.e. has a head injury with altered sensorium, is intoxicated, or has been given potent analgesics, the cervical spine must remain immobilized until a clinical examination becomes possible.[1]
Neurosurgeons or orthopaedic surgeons manage any detected injury. Today, most large centers have spine surgery specialists, that have trained in this field after their orthopedic or neurosurgical residency.
History and examination
A medical history and physical examination can be sufficient in clearing the cervical spine. Notable clinical prediction rules to determine which patients need medical imaging are Canadian C-spine rule and the National Emergency X-Radiography Utilization Study (NEXUS).[2]
The following is based on the NEXUS (National Emergency X-Radiography Utilization Study) criteria.[3]
Excluding a cervical spinal injury requires clinical judgement and training.
Under the NEXUS guidelines, when an acute blunt force injury is present, a cervical spine is deemed to not need radiological imaging if all the following criteria are met:
- There is no posterior midline cervical tenderness
- There is no evidence of intoxication
- The patient is alert and oriented to person, place, time, and event
- There is no focal neurological deficit (see focal neurological signs)
- There are no painful distracting injuries (e.g., long bone fracture)
Medical imaging
Choice of method
- In children, a CT scan of the neck is indicated in more severe cases such as neurologic deficits, whereas X-ray is preferable in milder cases, by both US[4] and UK[5] guidelines. Swedish guidelines recommend CT rather than X-ray in all children over the age of 5.[6]
- In adults, UK guidelines are largely similar as in children.[5] US guidelines, on the other hand, recommend CT in all cases where medical imaging is indicated, and that X-ray is only acceptable where CT is not readily available.[7]
Magnetic resonance imaging may be useful if it is necessary to exclude a ligament injury.[8] The indication for MR spine is a focal neurological deficit. Another indication for MR of the cervical spine is persistent mid-line neck pain or tenderness despite a normal CT in the awake patient.
Imaging settings
X-ray consists of a three view cervical x-ray series, adding a swimmer's view if the lateral doesn't include the C7/T1 interface.
CT scan should be thin slices, ideally 1.5 mm or less.[9] It should include first thoracic vertebra.[10]
Evaluation
CT scan or X-ray images are evaluated for the presence or absence of directly visible fractures. In addition, indirect signs of injury by the vertebral column are incongruities of the vertebral lines,[11] and/or increased thickness of the prevertebral space:[12]
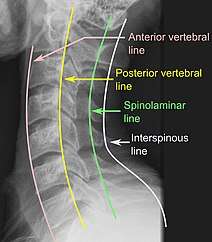 X-ray of normal congruous vertebral lines
X-ray of normal congruous vertebral lines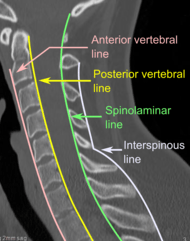

After imaging
If the patient is not expected to be clinically evaluable within 48–72 hours because of severe head or multiple injuries, they should remain immobilized until a time when such an examination is possible. A 64-slice CT with reconstructions does not entirely rule out ligamentous injury leading to instability, but is a practical means of identifying the majority of C-spine injuries in obtunded patients. MR C-spine suffers from frequent false-positives, limiting its usefulness. In these cases, a consultation with a Spine Surgery specialist is prudent.
See also
References
- Morris CGT, McCoy E (2004). "Clearing the cervical spine in unconscious polytrauma victims, balancing risks and effective screening". Anaesthesia. 59 (5): 464–482. doi:10.1111/j.1365-2044.2004.03666.x. PMID 15096241.
- Saragiotto, Bruno T; Maher, Christopher G; Lin, Chung-Wei Christine; Verhagen, Arianne P; Goergen, Stacy; Michaleff, Zoe A (2018). "Canadian C-spine rule and the National Emergency X-Radiography Utilization Study (NEXUS) for detecting clinically important cervical spine injury following blunt trauma" (PDF). Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD012989. ISSN 1465-1858.
- Hoffman JR, Wolfson AB, Todd K, Mower WR (1998). "Selective cervical spine radiography in blunt trauma: methodology of the National Emergency X-Radiography Utilization Study (NEXUS)". Ann Emerg Med. 32 (4): 461–9. doi:10.1016/s0196-0644(98)70176-3. PMID 9774931.
- Julie C Leonard (2018-02-12). "Evaluation and acute management of cervical spine injuries in children and adolescents". UpToDate.
- "Head injury: assessment and early management". National Institute for Health and Care Excellence (NICE). 2014. Updated in June 2017
- "Traumamanual". Region Skåne. Last updated: 2018-03-29
- Amy Kaji, Robert S Hockberger (2018-05-24). "Evaluation and acute management of cervical spinal column injuries in adults".
- Jaeseong, Jason (2015). "The utility of flexion–extension radiography for the detection of ligamentous cervical spine injury and its current role in the clearance of the cervical spine". Emergency Medicine Australasia. doi:10.1111/1742-6723.12525. PMID 26685877.
- Tins, Bernhard (2010). "Technical aspects of CT imaging of the spine". Insights into Imaging. 1 (5–6): 349–359. doi:10.1007/s13244-010-0047-2. ISSN 1869-4101. PMC 3259341. PMID 22347928.
- Mark Karadsheh. "Cervical Spine Trauma Evaluation". Orthobullets. Updated: 4/24/2019
- Raniga, Sameer B.; Menon, Venugopal; Al Muzahmi, Khamis S.; Butt, Sajid (2014). "MDCT of acute subaxial cervical spine trauma: a mechanism-based approach". Insights into Imaging. 5 (3): 321–338. doi:10.1007/s13244-014-0311-y. ISSN 1869-4101. PMC 4035495. PMID 24554380.
- Rojas, C.A.; Vermess, D.; Bertozzi, J.C.; Whitlow, J.; Guidi, C.; Martinez, C.R. (2009). "Normal Thickness and Appearance of the Prevertebral Soft Tissues on Multidetector CT". American Journal of Neuroradiology. 30 (1): 136–141. doi:10.3174/ajnr.A1307. ISSN 0195-6108. PMID 19001541.